Only one COVID-19 inoculation has gained FDA approval (Comirnaty) in the US. More recently, the medication has gained Emergency Use Authorization (EUA) from the FDA for children between ages 5-11.
But how many are aware that Comirnaty is not actually available in the US?
I’ll get into that later. For now, it’s important to note that all COVID-19 inoculations currently being given in the US must still be regarded as experimental, and recipients of these products must therefore be regarded as trial participants. And that’s not because you can’t actually get the FDA-approved product in the US. But because, as I’ll also explain later, the initial Pfizer clinical trials for their FDA-blessed COVID serum are not scheduled to conclude for several more years. This is a fact that can be easily verified through the FDA’s approval letter, which includes the Comirnaty clinical trial schedule.
Informed consent mandates that subjects participating in a medical experiment must be informed of potential risks and benefits of the study prior to participating in the clinical trial. But the FDA’s guidelines for informed consent are not being followed. As unwitting participants in COVID inoculation clinical trials, and every patient receiving an injection in the US should be made aware of the elements of informed consent prior to injection.
But are these injections safe? Are they effective? It depends on whom you ask. It depends on what you read. It depends on what you watch. But mostly it depends on how well your life experiences have prepared and enabled you to detect and avoid the odor of clown shit.
It is a dangerous proposition to rely exclusively on mainstream media for answers. Many outlets read from the same script and will promote whatever agenda serves corporate and/or political interests—not necessarily what benefits the public.
In fact, carnival barkers from disparate, major networks often unify to program viewers with rhetoric, slanted coverage, and outright propaganda. ABC, CBS, FOX, NBC, etc.—they all blow the same whistle.
Conspiracy theory? The brief video presented below exposes the Operation Mockingbird collective.
Even science itself must be viewed with a healthy dose of skepticism.
Marcia Angell, faculty member of Global Health and Social Medicine at Harvard Medical School and a former Editor in Chief of The New England Journal of Medicine, observed, “It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as editor of The New England Journal of Medicine.”
Dr. Richard Horton, the current editor-in-chief of the Lancet – considered to be one of the most well respected peer-reviewed medical journals in the world, writes, “The case against science is straightforward: much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with small sample sizes, tiny effects, invalid exploratory analyses, and flagrant conflicts of interest, together with an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness.”
In Celia Farber’s article Was the COVID-19 Test Meant to Detect a Virus? Dr. David Rasnick, bio-chemist, protease developer, and former founder of an EM lab called Viral Forensics, says one of the ways to distinguish truth from deception in contemporary “science” is to track what gets removed. “For example,” Rasnick said, “there was apparently an English abstract online at PubMed out of China that rendered the entire COVID testing industrial complex baseless and absurd.”
“[The paper] estimated that if you’re testing asymptomatic people, up to 80% of positives could be false positive. That was kind of shocking, so shocking that PubMed had to withdraw the abstract even though the Chinese paper appears to still be published and available,” Rasnick said.
And if you’re looking for answers from Wikipedia, be forewarned of “Astroturf,” or fake grassroots movements funded by political, corporate, or other special interests. These subversive tactics can very effectively manipulate and distort media messages, including Wikipedia entries.
Steve Kirsch, Executive Director, Vaccine Safety Research Foundation, provides a stunning example Wikipedia’s manipulations. In his piece How Wikipedia transformed me into an evil person in just 4 days, Kirsch notes, “After I spoke out against the vaccines, Wikipedia totally changed my profile over time from a good guy into a menace to society.”
Veteran investigative journalist Sharyl Attkisson further discusses the astroturfing practice in a revealing 2015 Ted talk, presented below.
Research vs Inquiry
Unfortunately, most people will likely spend less than half an hour researching COVID injections. And there is a difference between research and simply asking your doctor or a friend if the shots are safe and effective and leaving it at that.
The latter is merely inquiry—such as asking a cook if Stevia a good, natural sugar substitute, accepting the answer, and then going off and baking a batch of cookies with the sweetener.
But unless you followed up with actual research, you wouldn’t discover that all “Stevia” sold in grocery stores is produced in China and processed with toxic chemicals. When you look at the refinement process, Stevia is no more natural than Aspartame, Splenda, NutraSweet, Equal, Sweet N Low, etc. Furthermore, Stevia can become a carcinogenic, and it is not recommended for use of nursing and pregnant women.
Even professional chefs are likely to be unaware of this information. Chefs generally spend their valuable time cooking ingredients, not researching them.
Professionals are often loathe to admit ignorance of matters germane to their field. But, rather than take the time to research these topics themselves, they, like consumers, will simply regurgitate whatever they have heard in major media or have been handed down by Corporate (the same Corporate that helps feed the Mockingbird). It’s a convenient process that often results in the dangerous propagation of groupthink.
Educational Expenses
Before buying a car, most people will devote hours to reading reviews, scrutinizing and test-driving multiple vehicles before committing to purchase. They will inquire about everything from safety, to fuel efficiency, to warranty to cost—and the process might take days, weeks or even months.
Yet, these same diligent consumers are likely to spend about as much time as a handful of commercial breaks researching the experimental serum they’re about to inject into their child’s body.
But many people don’t want to be burdened with information—they just want to be told what to do.
Which, in many cases, is understandable. Information takes time to process. It demands critical thinking and intellectual honesty. The gathering of knowledge may lead to conclusions anathema not only to family and friends, but also to one’s own illusion of truth. Revelations can be taxing mentally physically, and socially.
Any knowledge worth knowing, however, comes at a price.
Those unwilling to pay the price will drift into a state of blissful ignorance. “Don’t make me think about it, just tell me what to do,” they will plead. These circus patrons will be well-protected from the labor of discovering and consequences of knowing truth. Passivity is far too formidable an enemy for these individuals to defeat.
This is especially poignant when it comes to medicine, a field that takes decades of training and experience in which to achieve proficiency. Not having comparable skill and knowledge, we rely on medical professionals, academics, the government, and media to advise us on matters related to our health and fitness.
Many will attempt to escape the emotional guilt and responsibility that may follow medicine gone awry by outsourcing their knowledge to such entities. “But the FDA assured me it was safe,” victims will sob following an adverse event. “It’s not my fault that my child has myocarditis—Dr. Gupta said it was rare!” they will shriek. “Lester Holt never said anything about blood clots!” they will cry.
Yes, knowledge worth knowing comes at a price. But so too does the lack of knowledge worth knowing.
Selling Out
Today’s physician is much different than that of yesteryear. Private practices are dwindling as doctors are absorbed into large networks and groups that ultimately serve the interests of stockholders, not patients.
Consider the American Medical Association’s AMA COVID-19 GUIDE: Background/messaging on vaccines, vaccine clinical trials & combatting vaccine misinformation. Incorporating vocabulary such as “talking points,” “narrative,” and “message development and dissemination,” this publication aims to transform the medical practitioner into little more than a shill for Big Pharma.
Of course, shilling for Big Pharma has its benefits. Several of Canada’s largest legacy media companies failed to reveal nearly $2 million worth of Pfizer Pharmaceuticals funding that a leading pediatrics professor from Alberta received while pushing for vaccination of 5-11-year-olds through their channels.
There is little doubt that the AMA will soon suggest that physicians begin cold-calling their patients. The Diamond Club awaits.
But it’s not difficult to understand why the vast majority of medical professionals support COVID inoculations—outwardly, at least. To speak against the shot is to spread “misinformation” and risk losing a career—a career that cost countless hours of study, training and financial investment. And in many cases educational loan obligations are still being repaid.
To suggest that some patients may not need to be inoculated due to prior infection, allergies, safety or religious concerns may be deemed misinformation. Misinformation has become any statement that contradicts the narrative that everyone must be inoculated—no exceptions. Even animals at the Cincinnati Zoo are being injected with Covid serum. Where are the clinical trials for a giraffe? What’s next? House plants?
Ultimately, the AMA is not responsible for your family’s health and well-being. You are.
Who will pay physically, emotionally, and financially for any adverse reaction or death brought about by a COVID inoculation? The AMA? FDA? CDC? Your employer? Pfizer? Nope. You and your family will carry that crushing burden for a lifetime.
While most are not equipped with the training and expertise of a medical professional, most are able to read and comprehend papers written by these people. Most have the ability to interpret data charts, and most have the wherewithal to recognize trends.
It is critical to understand that what science believes is unrelated to how nature behaves. And it is certainly unrelated to how people behave. Take the time and energy to empower yourself with potentially life-saving knowledge.
What’s in a Name?
Pfizer? BioNTech? Comirnaty? What’s the difference? Only one of these medicines, Comirnaty, has actually received FDA approval. Pfizer, working with Corminarty, has made that particular brand of serum available only outside of the U.S. Comirnaty is not produced for a U.S.-licensed label anywhere in the FDA’s jurisdiction. If you live in America, you simply cannot get it domestically.
Why? Follow the money, not the science.
In its Comirnaty approval letter, the FDA notes that the licensed Pfizer Comirnaty vaccine and the existing, Emergency Use Authorization (EUA) Pfizer vaccine are “legally distinct.” The agency further stresses that their differences do not “impact safety or effectiveness.”
Same lady, different dress. But if dresses were armor, the woman with fashion designed by BioNTech would enjoy legal indomitability.
It all comes down to liability. Provided under EUA, all COVID serums enjoy a liability shield. Anyone experiencing harm from taking the product would not be able to sue the manufacturer for damages. FDA licensed adult vaccines, however, including the Comirnaty serum, are afforded no such protections.
“This is a unique situation where we as a company simply cannot take the risk if in … four years the vaccine is showing side effects,” Ruud Dobber, a member of Astraeneca’s senior executive team, told Reuters.
The FDA’s reissued Comirnaty approval letter acknowledges the existence of “a significant amount” of Pfizer’s current BioNTech serum—a surplus. In giving Pfizer’s newer (but “insufficiently stocked”) Comirnaty serum its blessing, the agency is allowing Pfizer to unload stockpiles of old, unused BioNTech product on unsuspecting consumers.
While parents believe their kids are receiving an FDA approved product, their sons and daughters will actually be injected with an unlicensed, experimental serum whose recipe had likely become outdated months before.
Thus, in licensing Comirnaty rather than BioNTech, the FDA gives Pfizer liability protection while affording the company an opportunity to clear out aging product. More importantly, however, FDA approval not only works to instill public confidence in the experimental product, but it also provides cover for the imposition of COVID serum mandates at all levels of society.
The FDA recently granted EUA for Comirnaty for 5-11 year olds.
Steve Kirsch, Executive Director, Vaccine Safety Research Foundation, explains, “Once Comirnaty is fully approved in kids, then Pfizer gets liability waiver on all age groups due to a ‘feature’ in federal law for child vaccines (NCVIA). At that time, they are done. They can market the COVID vaccine products under full approval for all age groups and face no liability when it kills or disables you.”
“This is why they are focused on the kids. This is why there is a reformulation at a 1/3 dose and they changed the buffer and the storage conditions (low temperatures not required). All of these will weaken the protection, but result in a safer vaccine (since it is ineffective).”
This bait and switch of formulations will keep adverse events from manifesting in the general child population until Comirnaty is fully approved for 5-11 year olds. A significant showing of adverse reactions prior to full product approval could jeopardize the FDA’s blessing.
Fast Forward
Most parents would certainly be bothered to discover other disturbing aspects of Pfizer’s Comirnaty experimental serum. The original Comirnaty approval letter reveals the following clinical trial completion dates:
Deferred pediatric Study C4591007 to evaluate the safety and effectiveness of COMIRNATY in infants and children 6 months to <12 years of age.
Final Protocol Submission: February 8, 2021
Study Completion: November 30, 2023
Final Report Submission: May 31, 2024
Study C4591009, entitled “A Non-Interventional Post-Approval Safety Study of the Pfizer-BioNTech COVID-19 mRNA Vaccine in the United States,” to evaluate the occurrence of myocarditis and pericarditis following administration of COMIRNATY.
We acknowledge the timetable you submitted on August 21, 2021, which states
that you will conduct this study according to the following schedule:
Final Protocol Submission: August 31, 2021
Monitoring Report Submission: October 31, 2022
Interim Report Submission: October 31, 2023
Study Completion: June 30, 2025
Final Report Submission: October 31, 2025
Study C4591021 substudy to describe the natural history of myocarditis and pericarditis following administration of COMIRNATY.
We acknowledge the timetable you submitted on August 21, 2021, which states
that you will conduct this study according to the following schedule:
Final Protocol Submission: January 31, 2022
Study Completion: March 31, 2024
Final Report Submission: September 30, 2024
Study C4591036, a prospective cohort study with at least 5 years of follow-up for potential long-term sequelae of myocarditis after vaccination (in collaboration with Pediatric Heart Network).
We acknowledge the timetable you submitted on August 21, 2021, which states
that you will conduct this study according to the following schedule:
Final Protocol Submission: November 30, 2021
Study Completion: December 31, 2026
Final Report Submission: May 31, 2027
Study C4591007 substudy to prospectively assess the incidence of subclinical myocarditis following administration of the second dose of COMIRNATY in a subset of participants 5 through 15 years of age.
We acknowledge the timetable you submitted on August 21, 2021, which states
that you will conduct this assessment according to the following schedule:
Final Protocol Submission: September 30, 2021
Study Completion: November 30, 2023
Final Report Submission: May 31, 2024
Study C4591007 substudy to evaluate the immunogenicity and safety of lower dose levels of COMIRNATY in individuals 12 through <30 years of age.
Final Protocol Submission: September 30, 2021
Study Completion: November 30, 2023
Final Report Submission: May 31, 2024
Study C4591014, entitled “Pfizer-BioNTech COVID-19 BNT162b2 Vaccine Effectiveness Study – Kaiser Permanente Southern California.”
Final Protocol Submission: March 22, 2021
Study Completion: December 31, 2022
Final Report Submission: June 30, 2023
My, oh myocarditis! According to the trial schedule for the FDA-approved serum, the latest we should expect to have a final study report (potential long term effects) submitted to the FDA would be May 31, 2027. The earliest report (efficacy study C4591014) is not due for submission until June 30, 2023!
But, out of the goodness of it’s jabbed and now-inflamed heart, the FDA granted approval and deferred these reports, presumably in the interest of ahem—public health.
An expedited drug approval from the FDA takes approximately 7.1 years, while Pfizer’s product was able to receive the blessing in a few short months. Would you fly on an airplane that was built in accordance with a similar production timeline? The inoculated have boarded a plane that is being built while it is in the air.
Efficacy
It should first be noted that none of the COVID serum clinical trials are designed to detect a reduction in any serious outcome such as hospitalizations, intensive care use, or deaths. They are merely designed to evaluate rate of infection among trial participants.
In terms of efficacy, what does a 12-15 year-old stand to gain from getting the experimental serum? We’ll first look at Susceptibility to SARS-CoV-2 Infection Among Children and Adolescents Compared With Adults: A Systematic Review and Meta-analysis for answers.
In this research, a total of 32 studies comprising 41 ,640 children and adolescents and 268 ,945 adults met inclusion criteria, including 18 contact-tracing studies and 14 population screening studies. The pooled odds ratio of being an infected contact in children compared with adults was 0.56.
The Delta variant is said to be 50% to 60% more transmissible than the original. So, let’s for the sake of argument adjust the probability of infection by 60%. Thus, the pooled odds ratio of being an infected contact in children compared with adults was 0.9.
Pfizer has boasted that its experimental serum demonstrated 95% relative efficacy in the company’s clinical trials involving adolescents 12 to 15 years of age (section 18.2).
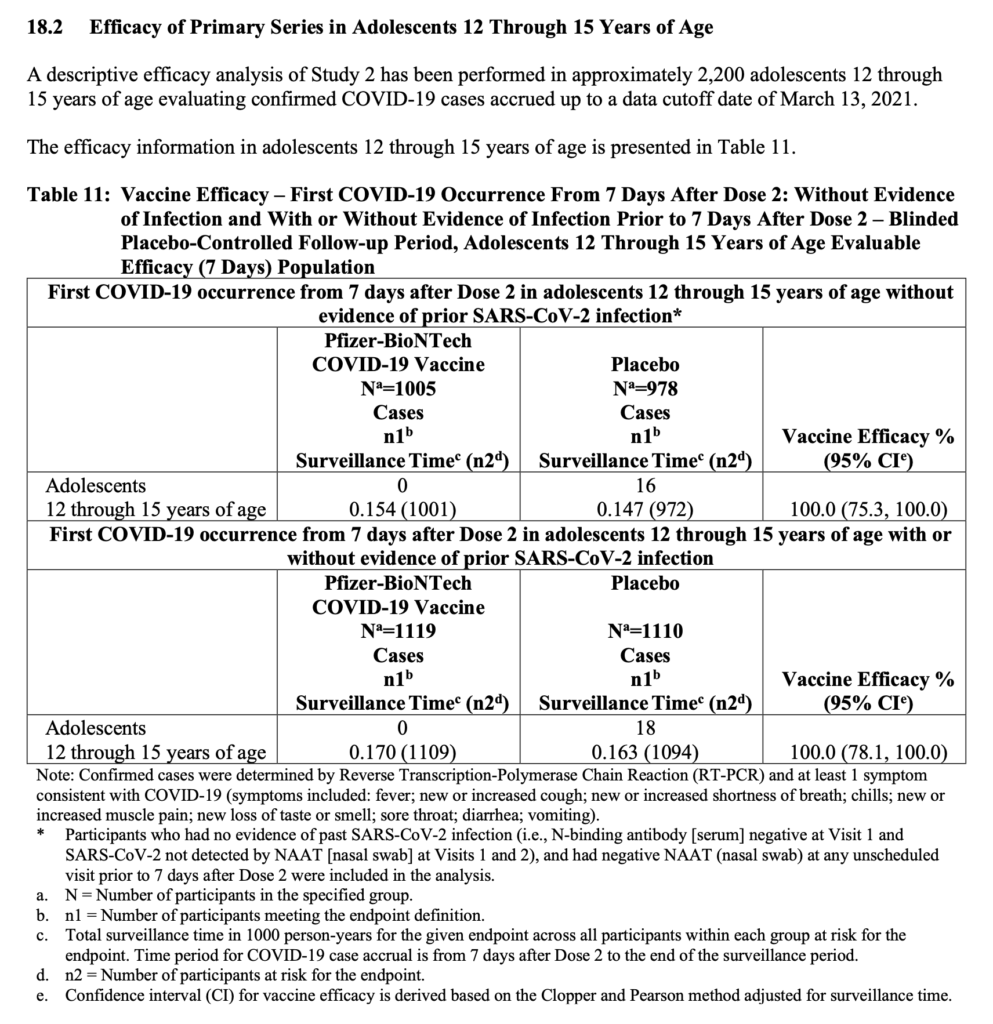
95% efficacy seems pretty impressive, right?
But this percentage is being applied to relative risk reduction, not absolute risk reduction. Absolute risk reduction, which is a key finding, was not reported.
The difference between efficacy and effectiveness is the difference between outcomes observed and reported in a controlled setting, such as a research trial, and those found in an uncontrolled, real world context. This differentiation is further applied to relative risk reduction versus absolute risk reduction.
In discussing the implications of efficacy (relative risk reduction) versus effectiveness (absolute risk reduction), Dr Alex Kennerly Vasquez reveals the true benefit afforded by the Pfizer and Moderna COVID injections:
Pfzier/BioNTech vaccine BNT162b2
- Relative risk reduction = 95%;
- Absolute risk reduction = 0.7%
Moderna vaccine mRNA-1273
- Relative risk reduction = 94%;
- Absolute risk reduction = 1%
Thus, in terms of contracting COVID, Pfizer’s own studies indicate that in getting fully inoculated, patients will gain an absolute risk reduction of only .7% following injection.
Safety
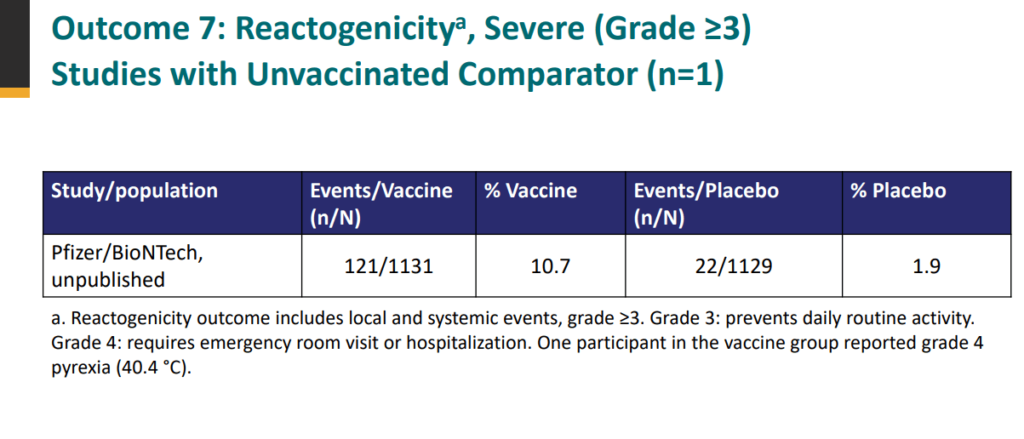
According to the review document submitted by Pfizer to the FDA, 1 in every 9 children in the trials suffered a serious adverse event (SAE) to the shot. An SAE is an event in which at least one criterion was met: caused death, is life-threatening, requires hospitalization or prolongation of existing hospitalization, results in persistent disability/incapacity, a congenital anomaly/birth defect.
Kids who were inoculated had nearly six times the risk of a SAE occurring in the two-month observation period compared to children who did not receive the serum. Therefore, there were almost seven times more SAEs observed in the inoculated group than there were Covid-19 cases in the uninoculated group.
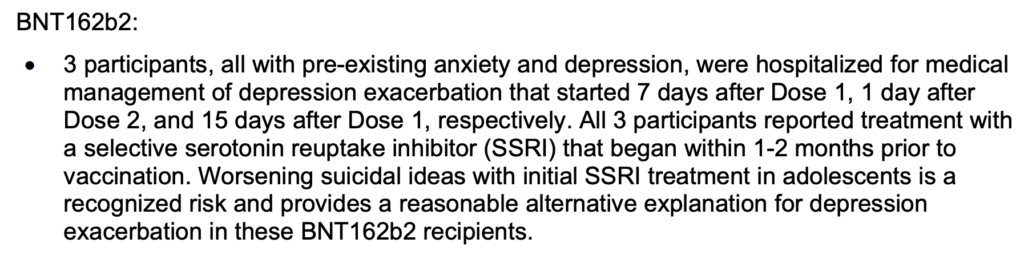
Of these reported SAEs, four children had such severe depression that they were hospitalized shortly after vaccination (in the first 7 days after the first dose, in the second only one day after the second dose, and in the third 15 days after the first dose, respectively). Thus, one in every 350-400 children who are vaccinated might suffer from severe depression and need hospitalization.
Nothing to See Here
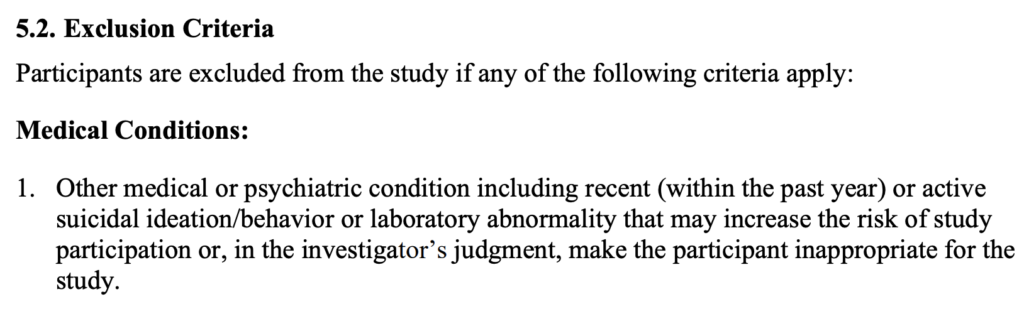
Pfizer explained that the psychologically affected children’s condition was a result of pre-existing diagnoses of anxiety and depression. They reasoned that the medication the kids were placed on 1-2 months prior to the study was responsible for the SAEs they experienced. Pfizer’s own trial protocol, however would have excluded these children from the study.
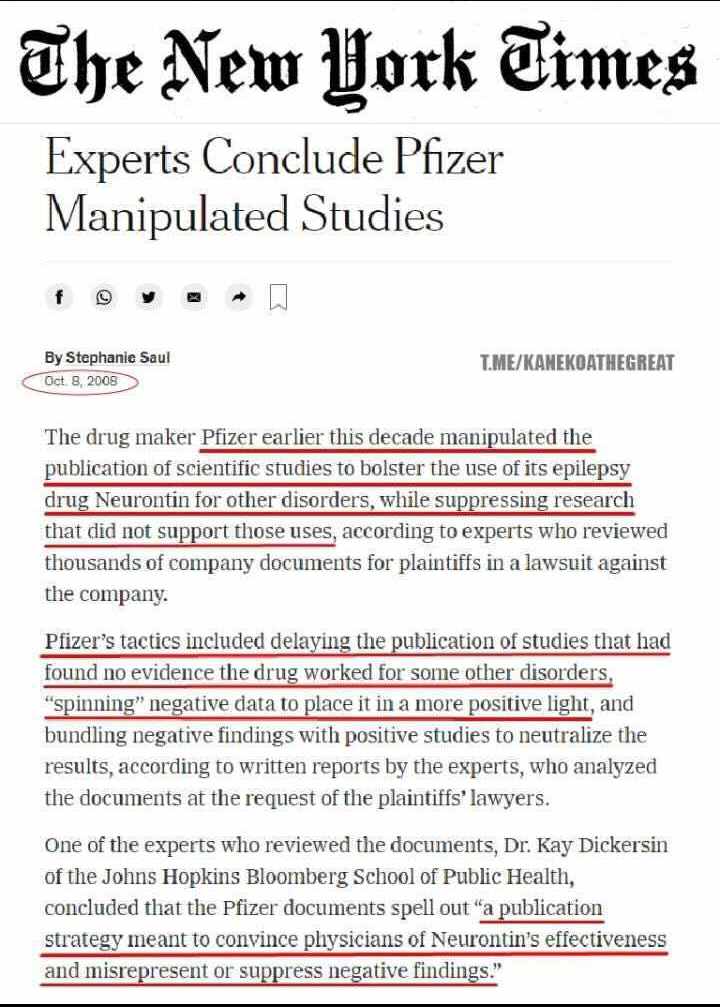
There have been serious allegations made that Pfizer manipulated study data and committed serious violations in order to gain EUA for their product. The case of 12-year-old clinical trial participant Maddie De Garay is particularly troubling. This unfortunate trial participant was paralyzed less than 24 hours after vaccination. Yet, Pfizer’s report presented De Garay’s adverse event as “abdominal pain,” with no mention of her paralysis, and Pfizer did not report this to the FDA. The FDA knew about the case by June 23, 2021 or earlier, but as of July 10 has not yet made any contact with the family to investigate what happened.

Why has the FDA not acted on the De Garay case? Because if they acknowledged that it was not reported that a perfectly healthy twelve- year-old was disabled less than 24 hours after getting inoculated, it would make them look bad. They would have to revoke the EUA, which would also make them look bad. So, rather than doing the right thing, the FDA turns a blind eye to a paralyzed twelve-year-old girl (who, as of this writing, is 13).
It is also concerning that Pfizer and Moderna purposefully dissolved their placebo groups during the trial, after the untested vaccines were given emergency use authorization. This violated the scientific purpose—to test whether the vaccine has any efficacy; any actual benefit and/or safety issues. Nearly all the control group were then given the serum following EUA.
There are other issues with Pfizer’s trial data. In fact, several physicians have signed a declaration stating, among other things, that Pfizer’s trial data are:
- Misleading, because these numbers pertain to relative, not absolute efficacy.
- Specious, because they refer to an arbitrarily defined, clinically meaningless evaluation endpoint, whereas no efficacy at all has been demonstrated against severe disease or mortality.
- Most likely altogether fraudulent.
Further support of the physicians’ concerns can be found in The BMJ (mostly referred to as the British Medical Journal) investigative report “Covid-19: Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial.”
Among the report’s allegation’s, the Pfizer clinical trial was tainted by the following:
- Poor lab management, patient safety, data integrity, needles discarded incorrectly
- Staff and patients unblinded to trials with placebos, directors failed to quantify errors
- Data entry issues for severe symptoms
- Fears over FDA inspection, FDA understaffed
- Patients not monitored, poor follow up protocols & mislabeling
This Just In (Updated Nov 16, 2021)
As reported by Alex Berenson:
“In their initial safety report to the FDA, which contained data through November 2020, [Pfizer and its partner BioNTech clinical trial] researchers had said four placebo recipients and two vaccine recipients died, one after the first dose and one after the second. The July update reversed that trend. Between November 2020 and March 2021, 13 vaccine recipients died, compared to only 10 placebo subjects.”
“Further, nine vaccine recipients had died from cardiovascular events such as heart attacks or strokes, compared to six placebo recipients who died of those causes. The imbalance was small but notable, considering that regulators worldwide had found that the Pfizer and Moderna mRNA vaccines were linked to heart inflammation in young men.”
In addition, according to the FDA’s “Summary Basis for Regulatory Action,” a 30-page document explaining why on August 23 it granted full approval to Pfizer’s vaccine, Berenson further notes:
And buried on page 23 of the report is this stunning sentence:
From Dose 1 through the March 13, 2021 data cutoff date, there were a total of 38 deaths, 21 in the COMIRNATY [vaccine] group and 17 in the placebo group.
Pfizer said publicly in July it had found 15 deaths among vaccine recipients by mid-March. But it told the FDA there were 21 – at the same data cutoff end date, March 13.
21.
Not 15.
The placebo figure in the trial was also wrong. Pfizer had 17 deaths among placebo recipients, not 14. Nine extra deaths overall, six among vaccine recipients.
Could the discrepancy result from some odd data lag? Maybe, but the FDA briefing book also contains the number of Covid cases that Pfizer found in vaccine recipients in the trial. Those figures are EXACTLY the same as those Pfizer posted publicly in July.
Yet the death counts were different.
Pfizer somehow miscounted – or publicly misreported, or both – the number of deaths in one of the most important clinical trials in the history of medicine.
And the FDA’s figures paint a notably more worrisome picture of the vaccine than the public July numbers. Though the absolute numbers are small, overall deaths were 24 percent higher among vaccine recipients.
The update also shows that 19 vaccine recipients died between November and March, compared to 13 placebo recipients – a difference of almost 50 percent.
Were the extra deaths cardiac-related? It is impossible to know. The FDA did not report any additional details of the deaths, saying only that none “were considered related to vaccination.”
Further highlighting the role of the FDA in bringing trial data into question is their response to a FOIA request for data from the experiments.
Immediately following the agency’s approval of the Pfizer product, more than 30 academics, professors, and scientists from this country’s most prestigious universities requested the data and information submitted to the FDA by Pfizer to license its COVID-19 serum.
In response, The FDA has asked a federal judge to make the public wait until the year 2076 to disclose all of the data and information it relied upon to license Pfizer’s COVID-19 inoculation. Why would it take 55 years to release such important data and information to the general public? If the data supported the narrative that the drug was safe and effective, you would think that the FDA would release this information quickly, and with great fanfare.
The truth is, no one in the FDA can say with any degree of certainty just how safe these medicines are. Or, if they can say, they’re not doing so publicly.
This becomes clear when listening to the words of Dr Eric Ruben of Harvard University, as he joins fellow voting members of the FDA in discussing the approval of Pfizer’s product for 5-11 year-olds. Dr Rubin said, “We’re never going to learn how safe the vaccine is unless we start giving it, and that’s just the way it goes.”
Israel was one of the first nations to begin a program of mass inoculation. In an article in The Jerusalem Post titled Could mRNA COVID-19 vaccines be dangerous in the long-term?, Tal Brosh, head of the Infectious Disease Unit at Samson Assuta Ashdod Hospital, says, “There is a race to get the public vaccinated, so we are willing to take more risks.”
In the same article, Michal Linial, a professor of biological chemistry at the Hebrew University of Jerusalem, declares, “I won’t be taking it immediately – probably not for at least the coming year. We have to wait and see whether it really works.”
In reviewing data out of Israel since Linial’s interview from a year ago this month, it is doubtful that the professor would elect to receive the COVID inoculation at this point.
And Linial would in all likelihood be even more hesitant to take the jab if she were pregnant. After re-analyzing a study performed by the CDC, a peer-reviewed paper has called for the “immediate withdrawal of mRNA COVID vaccines for pregnant women, those breastfeeding, those of childbearing age and children.”
The shocking report estimated that unexpected termination of pregnancies actually occurred at a rate 7-8 times higher in vaccinated pregnant women than the rate in the baseline over the same time period.
The Case Against Cases
Before we discuss effectiveness, we must look at cases. What is a COVID case? In the Pfizer trials, a subject had to present at least one symptom in order to be considered COVID-positive.
But there is such a thing as a COVID carrier who is asymptomatic. Thus, if a trial participant contracted COVID but did not display any symptoms, that individual was not counted as either a breakthrough infection among the vaccinated or a regular infection among the placebo group.
When the COVID inoculations were announced, the promise was that they would prevent infection. But just because you can’t see the effects of infection does not mean that you have not been infected—much in the same way that taking Robitussin may help control your cough and fever, but it doesn’t mean that you haven’t contracted the flu.
So how is an asymptomatic or symptomatic individual able to verify if he’s been infected with COVID? In China they generally diagnose the virus with CT scans and one or two positive Polymerase Chain Reaction (PCR) tests.
In the US and elsewhere, we generally use the PCR test as the sole mechanism for diagnosing COVID.
But the PCR test was never meant to serve as a diagnostic tool, and it has different standards in different countries, and within countries, from lab to lab. You could test positive in one lab, drive down the street to another and have results come back negative. It all depends on the how sensitive the cycle threshold is set.
In his article, What Ever Happened to Sensible Medical Practice, Dr Edward Leyton writes, ” . . .depending on the cycle threshold (Ct) the test can be positive in people whose viral loads are minimal and who are asymptomatic. I don’t think that ever before in medicine have we relied on a test without so much as a mention of symptoms! Symptoms are the sine qua none of diagnosis. It’s symptoms -> health care practitioner -> examination/testing -> diagnosis. Not testing -> diagnosis! Public Health will probably tell you it was done that way because it was a pandemic; but frankly that’s no excuse to pervert course of medicine. So, we got inflated ‘cases’. What is a case? It’s just a positive PCR. Even the inventor of the PCR has stated his test was not to be used this way. These inflated case numbers began the fear cycle.”
Journalist Celia Farber asked Dr. David Rasnick, bio-chemist, protease developer, and former founder of an EM lab called Viral Forensics, what advice he has for people who want to be tested for COVID-19. “Don’t do it, I say, when people ask me,” he replied. “No healthy person should be tested. It means nothing but it can destroy your life, make you absolutely miserable.”
A positive test result can be destructive and make you miserable because it means quarantine for the testee, as well as close contacts—whether the individuals are symptomatic or asymptomatic.
According to a growing group of scientists, asymptomatic infections are a myth. A study published in Nature.com found, “Virus cultures were negative for all asymptomatic positive and repositive cases, indicating no ‘viable virus’ in positive cases detected in this study.”
Even the World Health Organization’s technical lead for CCOVID-19, Maria Van Kerkhove, confirms,“From the data we have, it still seems to be rare that an asymptomatic person actually transmits onward to a secondary individual.” View her response below when asked about the issue at a press briefing.
What would you do differently with symptomatic COVID than you would do with any other symptomatic viral infection? In both instances, you would likely stay home until you became asymptomatic. So why take the chance of drawing a false positive for COVID through a PCR test? It can only sentence you and those around you to an unnecessary self-imposed or mandatory confinement.
Effectiveness
No medication is 100% effective, and that has certainly the case with anti-COVID injections. Regardless, the initial promise of the COVID inoculations was that they were 100% effective in stopping infection and transmission of the disease. This claim has largely been memory-holed, but historical evidence of the assertion followed by time-tested outcomes can be seen below.
On the March 29, 2021 broadcast, of MSNBC’s Rachel Maddow Show, Maddow gushed over a CDC report on COVID-19 injections. “Instead of the virus being able to hop from person to person to person, potentially mutating and becoming more virulent and drug resistant along the way, now we know that the vaccines work well enough that the virus stops with every vaccinated person,” she enthused. “A vaccinated person gets exposed to the virus. The virus does not infect them. The virus cannot then use that person to go anywhere else. It cannot use a vaccinated person as a host to get more people.”
All fake news.
As the waning effectiveness of the COVID injections comes to light, the drug’s failure to live up to the initial promise of immunity for the inoculated has crippled that much-hyped narrative. This has led the peddlers of a faulty product to create a new narrative—one that helps explain away their product’s emerging and undeniable deficiencies. Thus, a new term has been born—a “Pandemic of the unvaccinated.”
Never before in history has the failure of a vaccine been blamed on people who did not take it.
But this is the difference between a “leaky” vaccine and a “sterilizing” vaccine. More on that later.
The most important thing for parents to think about right now is safety. We now know that COVID serum effectiveness has been grossly overstated. So how are we to know if similar misstatements have been promoted in terms of safety?
If a child should contract COVID, she can use the Cleveland Clinic’s COVID hospitalization predictor calculator to help predict that child’s chances of being hospitalized from the disease. But parents needn’t worry too much. According to CDC data, only .056% of hospitalizations of 5-17 year-olds since March 7, 2020 have been COVID-associated.
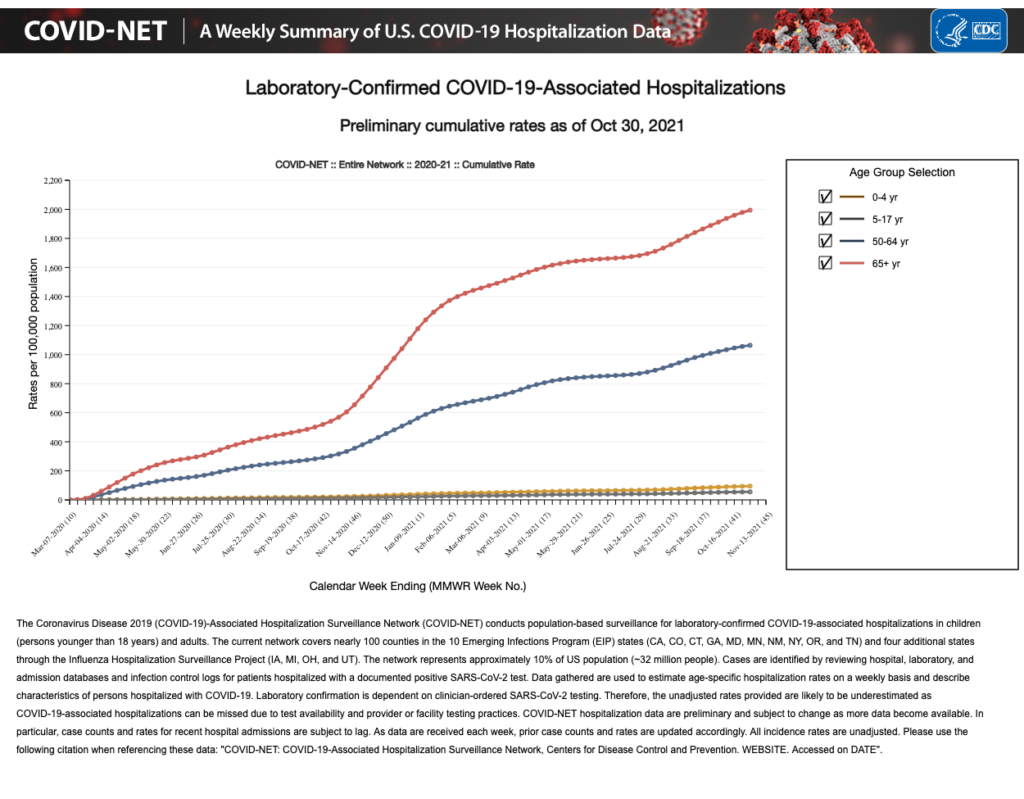
Furthermore, it should be noted that although COVID-19 has been reported as having considerable associated morbidity and mortality in children, reported hospitalization rates likely overestimate the true disease burden.
VAERS There’s Smoke . . .
Co-managed with the FDA, the CDC has established The Vaccine Adverse Event Reporting System (VAERS), a national early warning system to detect possible safety problems in U.S. licensed vaccines. VAERS accepts and analyzes reports of adverse events (possible side effects) following vaccination. Cases are self-reported and come from both clinicians, as well as the general public.
VAERS is the is the only present scientific way of measuring deaths and injuries from any vaccine – including the Covid-19 vaccine. It is the official primary data source that is used by the CDC and FDA to monitor adverse vaccine events, and it is not based on politics, and it has nothing to do with conservative or liberal opinions.
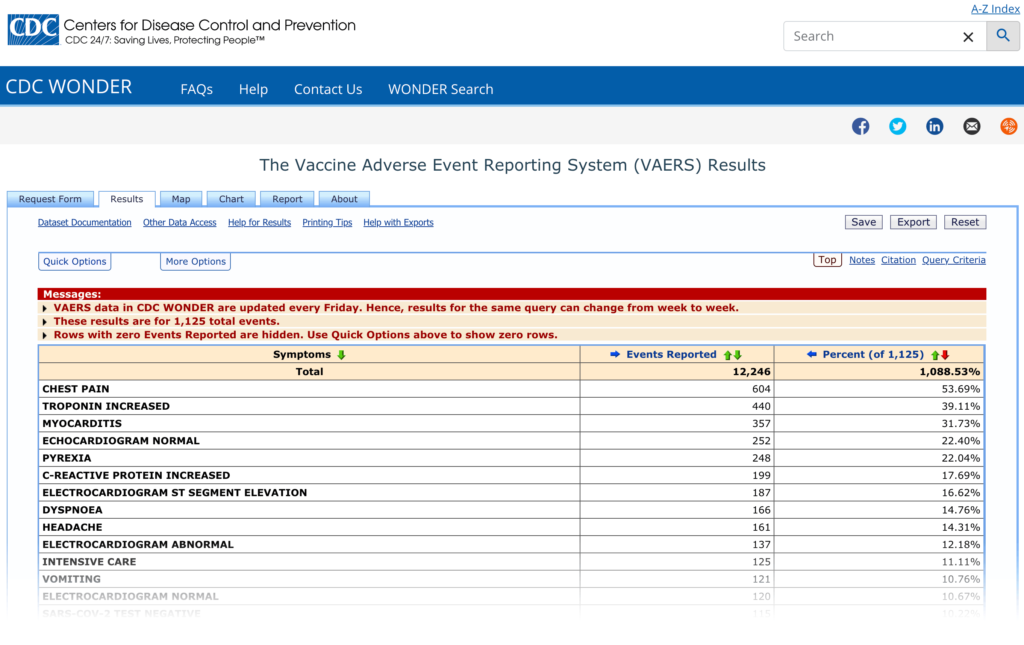
Data from VAERS reveals that children between the ages of 1-17 years old make up 1,125 of 32,612 hospitalizations (3.45%) directly attributable to COVID injections.
According to a well-known and oft-cited Harvard study on VAERS, fewer than 1% of vaccine adverse events are actually reported to the system.
My Oh Myocarditis!
In June, the FDA decided that the link between the mRNA vaccines and myocarditis, particularly in young males, was sufficiently clear that it revised its vaccine fact sheets to include a warning. Myocarditis is inflammation of the heart muscle, whereas pericarditis is inflammation of the protective sacs surrounding the heart. Once a heart cell is damaged by the serum, it is damaged forever. It does not replace itself with another heart cell—it is replaced by a scar.
According to the Myocarditis Foundation website, “Myocarditis is the 3rd leading cause of Sudden Death in children and young adults . . . After treatment, many patients live long, full lives free from the effects of myocarditis. For others, however, ongoing cardiovascular medication or even a heart transplant may be needed. Overall, myocarditis which can cause dilated cardiomyopathy, are thought to account for up to 45 percent of heart transplants in the U.S. today.”
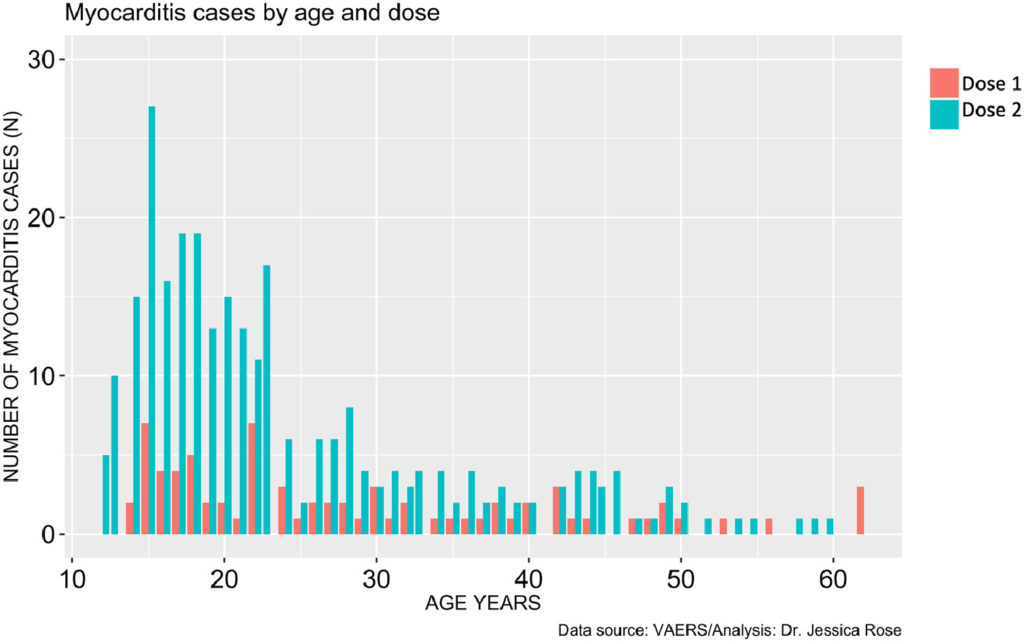
According to the CDC, reported cases of myocarditis have occurred usually a few days after getting the COVID-19 vaccine and mostly after receiving the second dose.
The CDC said that the heart risk has been reported after receiving either the Pfizer or Moderna COVID-19 vaccine mostly among young adults and male adolescents. In addressing this concern, the FDA has warned Moderna that the EUA approval of the company’s COVID-19 vaccine for adolescents as young as 12 years old may be delayed until early 2022.
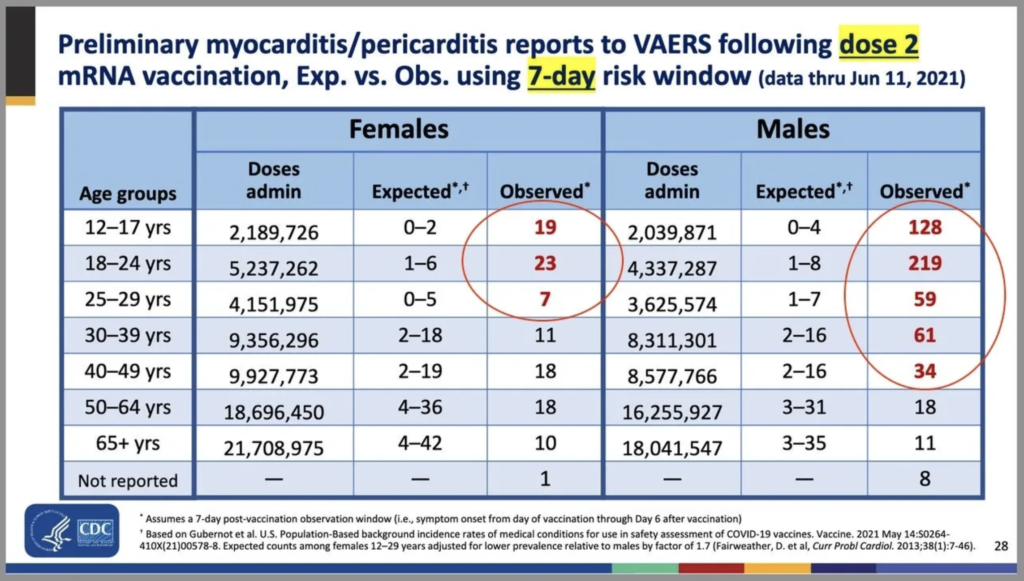
The CDC released data showing the incidence of “expected” versus “observed” incidences of myocarditis and pericarditis and found a significant increase in the observed rates. The graph below shows the higher rates in red (see table numbers circled in red).
Again, because VAERS has been shown to suffer from underreporting, accounting for cases of myocarditis and pericarditis should likely be even higher. This thesis is supported by research published in JAMA. That study found that boys aged 12-15 years vaccinated with their second shot of the mRNA vaccine, with no underlying medical conditions, were four to six times more likely to develop a cardiac adverse event, than ending up in hospital with COVID-19.
A report in ScienceDirect states, “Within 8 weeks of the public offering of COVID-19 products to the 12-15-yr old group, we found 19 times the expected number of myocarditis cases . . . over background myocarditis rates for this age group . . . 6 individuals died . . . Because of the spontaneous reporting of events to VAERS, we can assume that the cases reported thus far are not rare, but rather, just the tip of the iceberg.”
In addition, the authors conclude, “During phase III clinical trials for the mRNA COVID-19 products, safety was assessed based on a maximum observation period of 6 months. This is not adequate to assess long-term safety outcomes as it is a requirement, even in an accelerated timeline setting, to spend up to 9 months in Phase III trials. The typical timeline is up to 10 years for safety and efficacy assessment . . . It is vital to recall that children have a negligible risk for COVID-19 respiratory illness, and yet they are a high-risk group for myocarditis with vaccination.”
It should also be noted that there is a difference how myocarditis differs when caused by natural infection versus vaccine-induced infection. Cardiologist Dr. Peter McCullough explains, “Now there’s pre-clinical studies suggesting the lipid nanoparticles actually go right into the heart. The heart expresses the spike protein and the body attacks the heart.”
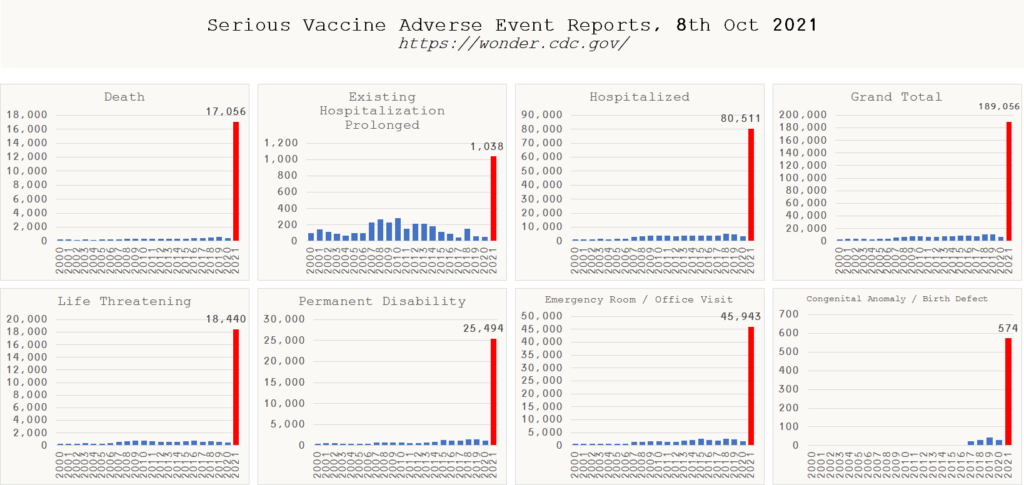
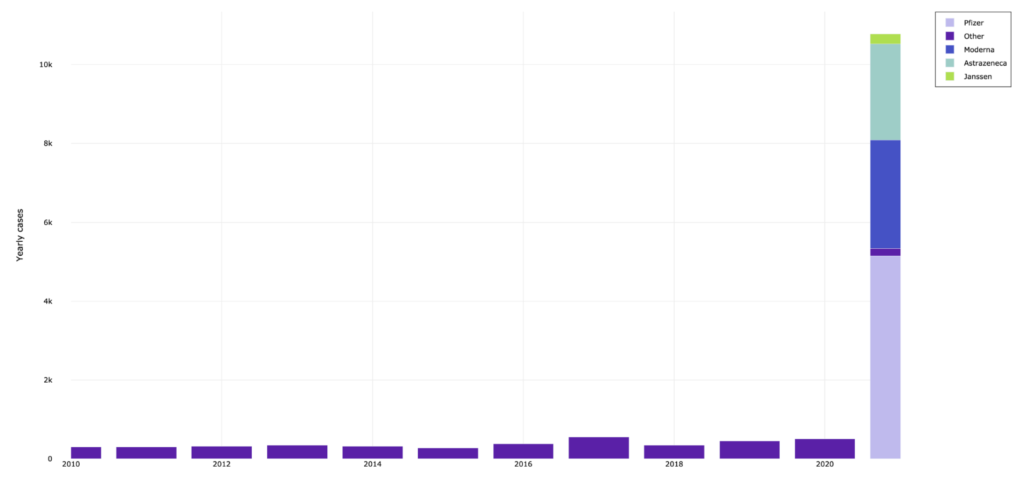
The vast underreporting in VAERS becomes all the more disturbing when, as of this writing, VAERS reports 17,000 Americans have died as a direct result of COVID injections – mostly from strokes, heart attacks and blood clots. Over 800,000 are reported injured, many of them hospitalized (over 83,000); many with life-threatening illness (over 18,000); many others permanently disabled (over 26,000).
The amount of deaths and significant injuries reported at VAERS is now dramatically higher than all vaccines in the past 30+ years combined. This has happened in only ten months.
Note the dramatic spike following the introduction of experimental injections in 2020.
In adjusting for underreporting, it has been estimated that at least 40,000 or more deaths have been caused by COVID vaccines and that over 2,000,000 people have been injured. Alarmingly, neither the FDA nor the CDC and their external committees will acknowledge VAERS underreporting—a damnable position for agencies tasked with conducting risk-benefit calculations. While underreporting is a well-known flaw in VAERS data collection, these agencies inexplicably refuse to publicly verify that VAERS is underreported or what the reporting factor is.
Dr. Jessica Rose has given an excellent VAERS presentation in which she discusses and interprets COVID VAERS data. Rose concludes that the serums are likely the cause of reported deaths, spontaneous abortions and anaphylactic reactions in addition to cardiovascular, neurological and immunological adverse events. Thus far, the accuracy of Rose’s findings have not been disputed.
But could VAERS data be a fluke? Some strange anomaly unrelated to the introduction of the experimental serums? While Rose does an excellent job discounting this theory in her video, additional evidence can be found overseas. EudraVigilance is the system for managing and analyzing information on suspected adverse reactions to medicines which have been authorized or being studied in clinical trials in the European Economic Area. Its vaccine mortality data parallels what is seen in VAERS.
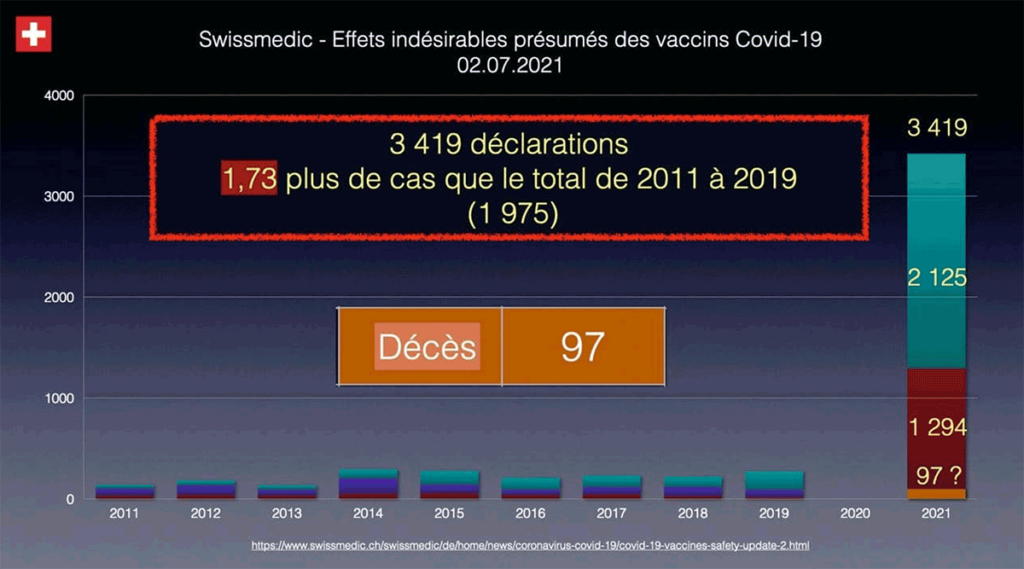
Swissmedic is the Swiss authorization and supervisory authority for drugs and medical devices. What does their data reveal? You don’t need to be able to read French to understand the message.
Tragedies Behind the Statistics
Soviet dictator Joseph Stalin famously observed, “One death is a tragedy; one million is a statistic.”
It can be easy to lose the personal stories of victims who succumb to experimental COVID serums in the numbers. While anecdotal, further evidence of inoculation dangers can be found on C19VaxReactions.com and Facebook.
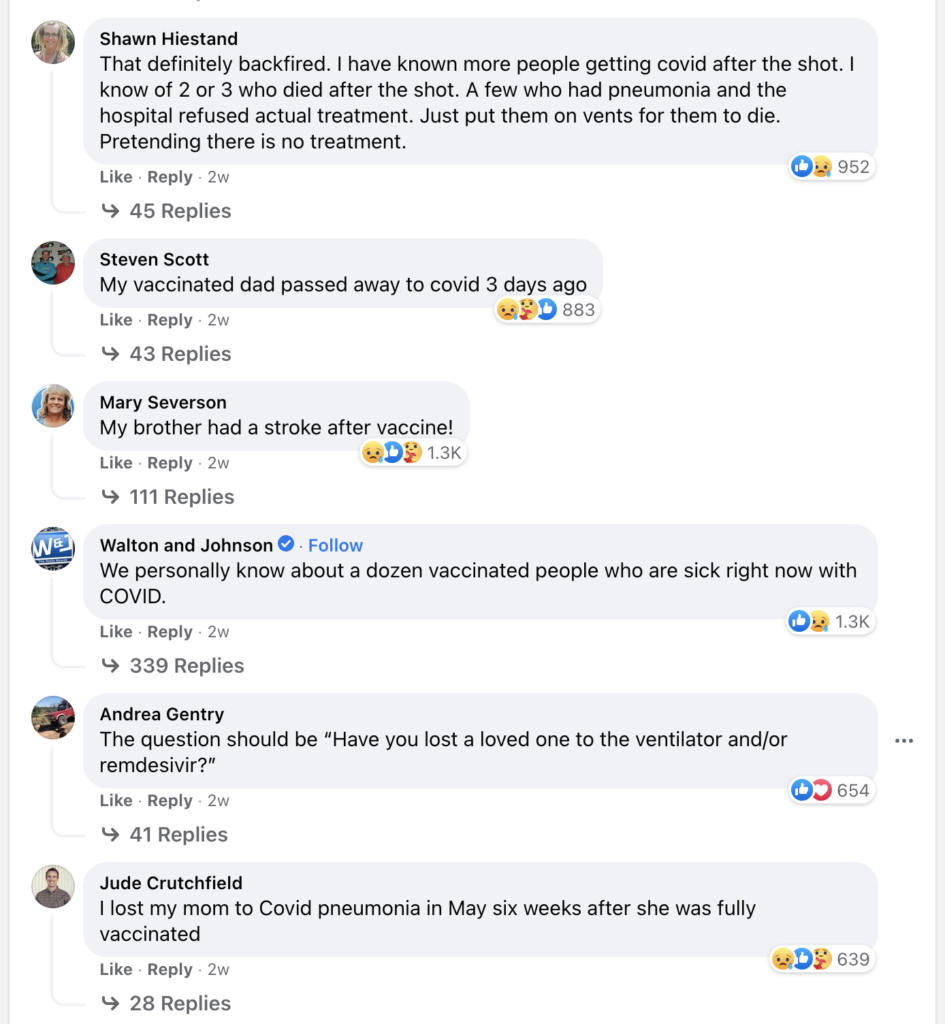
An ABC News Station in Detroit posted a request on Facebook for people to share their stories of unvaccinated loved ones who had died from COVID. They wanted to make a news story on this. What they got, however, was more than 250,000 comments from grieving and regretful posters, revealing a shocking amount of death and suffering these injections are causing.
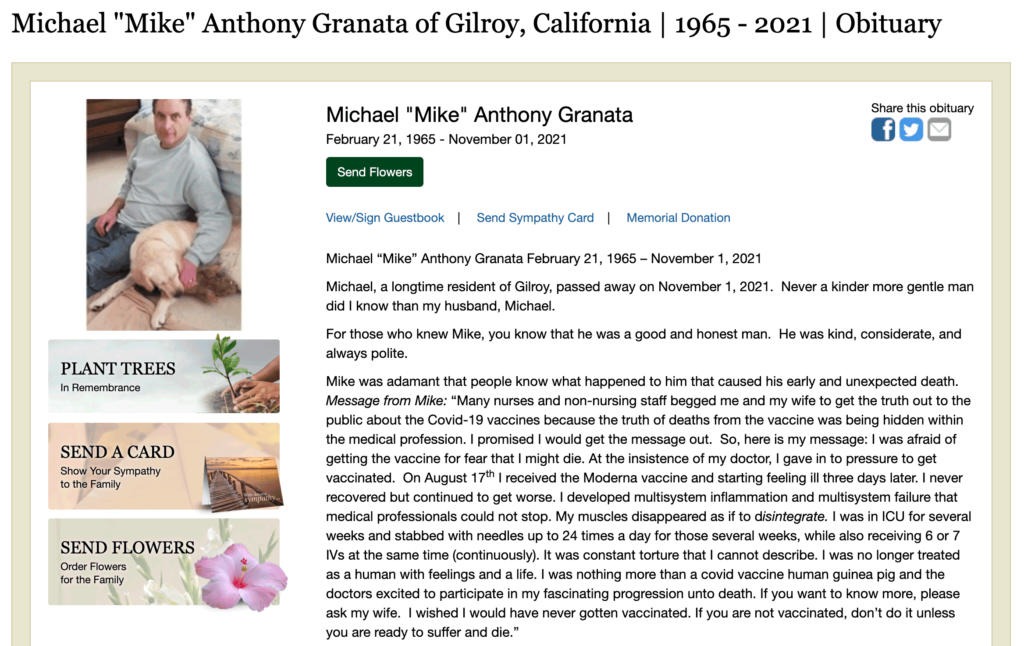
Mike Granata was adamant that people know what happened to him that caused his early and unexpected death. Granata’s full obituary includes details of his tortuous struggles following his Moderna inoculation.
In part, Granata wrote, “I was afraid of getting the vaccine for fear that I might die. At the insistence of my doctor, I gave in to pressure to get vaccinated . . . I was nothing more than a covid vaccine human guinea pig and the doctors excited to participate in my fascinating progression unto death.”
And then there’s the clown shit.
Do you notice anything peculiar about the Twitter posts below? Did you smell and avoid the droppings, or were you one of the unsuspecting dupes who stepped in them?

Please—take a moment to wipe the bottom of your shoe, if you must. But it will behoove you to be aware that there are a lot of burrito-eating clowns out there.
The Show Must Go On
In the last 40 years, the stopping condition for a vaccine is 25 to 50 deaths. Yet, according to the FDA, there is no stopping condition for these inoculations. What’s even more concerning is that not a single member of the medical establishment has a problem with the lack of a death-stopping condition on the experimental serums.
In 1976, the H1N1 vaccine was stopped after just 35 deaths. Today in 2021, more than 18,000 deaths caused by these injections is dismissed and even censored. If more than 18,000 deaths is not a stopping condition, what is? Apparently, there isn’t one. The faucet is to remain open despite the bathtub overflowing with water and flooding the living room below it.
With so many people already having been inoculated, it would be devastating for stakeholders to admit at this point that COVID shots are unsafe for humans. There would be widespread panic and fury, as well as demands for swift justice against culpable agents throughout the world. So don’t expect such an admission to come from the FDA, NIH, your pediatrician, or anyone else anytime soon.
More likely, a new product will be developed to supplant the shots. It will be heralded as a safer, more effective and convenient medical solution. And the current iteration of COVID injections will become memories of the past, but with a newfound future—one that will still demand unquestioned medical obedience.
Meanwhile, Big Pharma will continue to profit handsomely and without liability, regardless of the carnage wrought by their products.
Scrutinizing the Data
Using data reported on the CDC website at https://www.cdc.gov/vaccines/acip/me…bukuro-508.pdf p8 and https://www.cdc.gov/vaccines/aciameetings/downloads/slides-2021-06/05-COVID-Wallace-508.pdf p32, an unnamed actuary calculated the risk/benefit ratio for 12-17 year-olds. He determined the following:
Actuary Calculations
Hospitalizations Due to COVID Vaccine
Page 32: The CDC predicts that fully vaccinating 1 million male 12 to 17 year olds would prevent 5,700 cases, 215 hospitalizations and 2 deaths from COVID.
Number Needed to Treat (to prevent 1 COVID disease hospitalization), 1 Million/215 = 4651
Page 8: .2% of 12-15 year olds (and also of 16 to 25 year olds) required hospitalization and/or emergency room treatment after their 2. Pfizer dose and .1% after the 1st Pfizer dose.
Assuming 1st dose and 2nd dose hospitalizations/ER are not mutually exclusive (worst case scenario) Number Needed to Harm = 1/.2% = 500
OR assuming mutually exclusive categories and the .1% rate applies to ALL who received the 1st dose Total (hospitalized/ER on 1st, OR 2nd dose) = .3%.
Number Needed to Harm = 1/.3% = 333
Based on VAERS, “hospitalizations” account for a little more than 1/3 of the total of “hospitalizations or ER”. (July 2, 2021 VAERS in age group 6 to 17: 718 hospitalized + 1211 ER only = 1929. 718/1929 = 1/ 2.6 or 1/3 in round numbers. Thus, an adjustment factor of 3 was applied to the NNHs to derive a comparable basis. So, NNH is between 999 and 1500 for hospitalization. Note: There was no separate categorization between male and female, so this “unisex” version is used for both male and female.
Thus, the Pfizer vaccine is 3 to 5 times more likely to cause a 12 to 17 year old male to be hospitalized, than CDC predicts it will prevent hospitalization from the disease itself. (3 from 4651/1500 and 5 from 4651/999, rounded)
Page 32: The CDC predicts that fully vaccinating 1 million female 12 to 17 year olds would prevent 8,500 cases, 183 hospitalizations and 1 death from COVID.
Number Needed to Treat (to prevent 1 COVID disease hospitalization), 1 Million/183 = 5464
For 12 to 17 year old females, the Pfizer vaccine is 4 to 5 times more likely to cause hospitalization than CDC predicts to prevent it, by similar calculations. (4 from 5464/1500 and 5 from 5464/999, rounded).
Death with COVID Vaccine
Using the CDC’s figures on ‘at least partially vaccinated’ as of July 2, 2021, VAERS death data as of July 2:
Number Needed to Harm = 8,123,243 at least partially vaccinated/14 COVID vaccine deaths = 580,232
Male Number Needed to Treat (to save 1 life) = 500,000
Female Number Needed to Treat (to save 1 life) = 1,000,000
So 12-17 year old males are only 16% less likely to die from COVID, than their vaccine. Females aged 12-17 years old are 72% MORE likely to die from their vaccine than COVID itself. (16% from 500,000/580,232 and 72% from 1,000,000/580,232)
And what of 5-11 year-olds? According to a risk-benefit analysis done by risk-benefit expert Dr. Toby Rogers, “The Pfizer vaccine fails any honest risk-benefit assessment in connection with its use in children ages 5 to 11. The FDA’s risk-benefit analysis of Pfizer’s mRNA vaccine in children ages 5 to 11 is shoddy. It used tortured logic (that would be rejected by any proper academic journal) in order to reach a predetermined result that is not based in science.”
Rogers concludes, “We will kill 117 kids to save one child from dying from COVID in the 5 to 11 age range.” His analysis has been scrutinized and by over 22,000 readers, and no errors were reported.
A recent peer-reviewed paper also concluded that COVID shots are more likely to kill than the virus. “Most importantly, the clinical trials did not address long-term effects that, if serious, would be borne by children/adolescents for potentially decades,” the authors asserted.
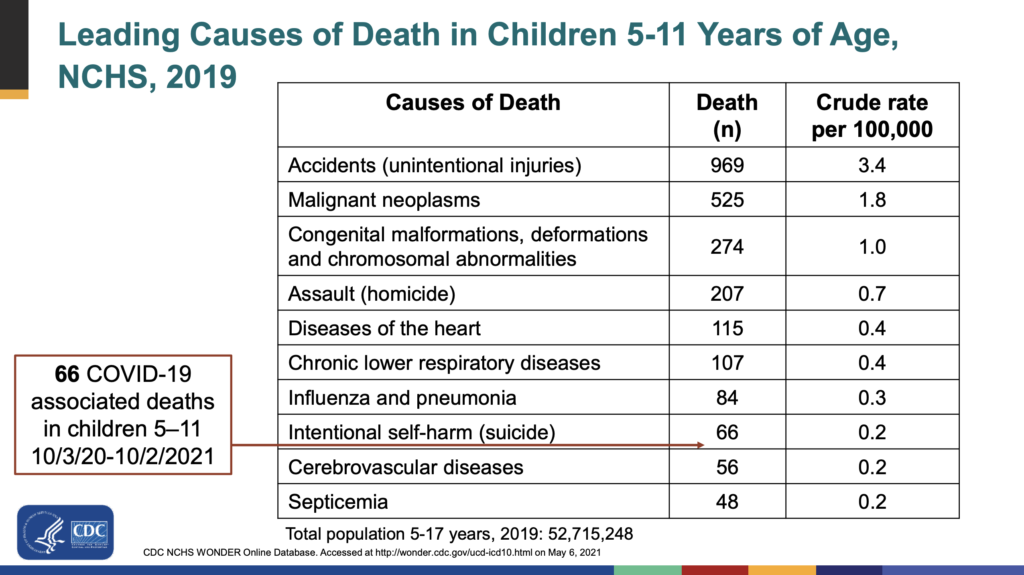
Now, let’s put COVID mortality rate for children 5-11 into perspective. In reviewing the CDC’s chart below, parents will come to understand that their kids will stand a far better chance of dying in a car accident on the way to get inoculated for COVID than he will from succumbing to the disease itself.
From the CDC’s own slide, presented at ACIP Meeting November 2, 2021 at the CDC:
- From 10/3/20 to 10/2/21
- 66 deaths *associated* with Covid (not all due to)
- Out of 28 million kids, aged 5-11
- Covid has risk of 0.000235714%
- Kids are fine 99.999764286% of the time
As seen in the graph below, statics reveal that COVID mortality in Great Britain actually closely mirrors a natural risk timeline by age. Note the COVID death rate in kids in this particular illustration.
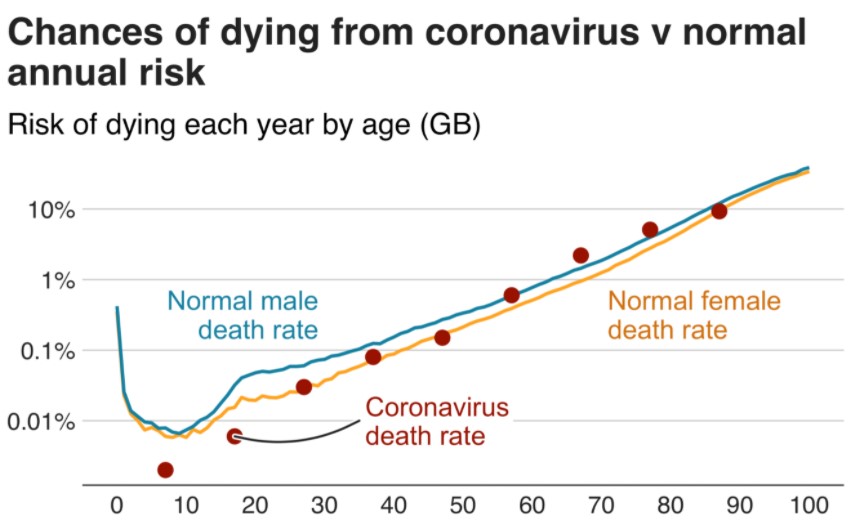
The estimated infection fatality rate (IFR) is close to zero for children and young adults. PANDA reports that the IFR for those <19 years is 0.003%. Levin reported that the estimated age-specific IFR was 0.002% at age 10 and 0.01% at age 25.
Comparatively, the American Council on Science and Health (ACSH) reported the IFR for males is as follows: 0-4 years, mean 0.003%, 5-9 years, mean 0.001%, 10-14 years, mean 0.001%, 15-19 years, mean 0.003%, 20-24 years, mean 0.006%.
The most updated data by the American Academy of Pediatrics showed that Children were 0.00%-0.26% of all COVID-19 deaths, and 7 [US] states reported zero child deaths. In 45 states reporting, only 0.00%-0.03% of all child Covid-19 cases resulted in death.
A recent systematic review reported severe COVID-19 occurred in 5.1% of children and adolescents with pre-existing conditions (comorbidities such as obesity and diabetes) and in 0.2% without. According to the CDC, on average, there were 4.0 additional comorbidities for 94% of those who died with COVID.
In his piece Why is Pfizer pushing an untested vaccine on children? researcher Techno Fog writes, “According to CDC data, children aged 5-14 years-old have accounted for only 161 COVID-19 deaths since the start of the pandemic. In comparison, this same group has experienced 194 pneumonia deaths. To put these numbers into perspective, the CDC cites over 530,000 COVID-19 deaths for the ages 65 years and up. As New York Magazine observed, ‘The Kids Were Safe from COVID the Whole Time.'”
The truth is, most people grossly overestimate their chances of succumbing to COVID. Use Johns Hopkins COVID 19 Risk Tool to determine your specific odds of dying from the disease.
Suppressing Therapeutics, Not COVID
Sadly, many COVID hospitalizations and deaths may have been prevented with the use of proven, safe and effective therapeutics such as Hydroxychloroquine (HCQ) and Ivermectin (IVM). Prescribed for decades, these drugs have been vilified in an effort to advance political and/or financial concerns.
Clinical trial data, coupled with other compelling evidence, clearly reveal the efficacy of these therapeutics. IVM is even included on the WHO list of Essential Medicines and has earned its inventors the Nobel Prize in Physiology or Medicine.
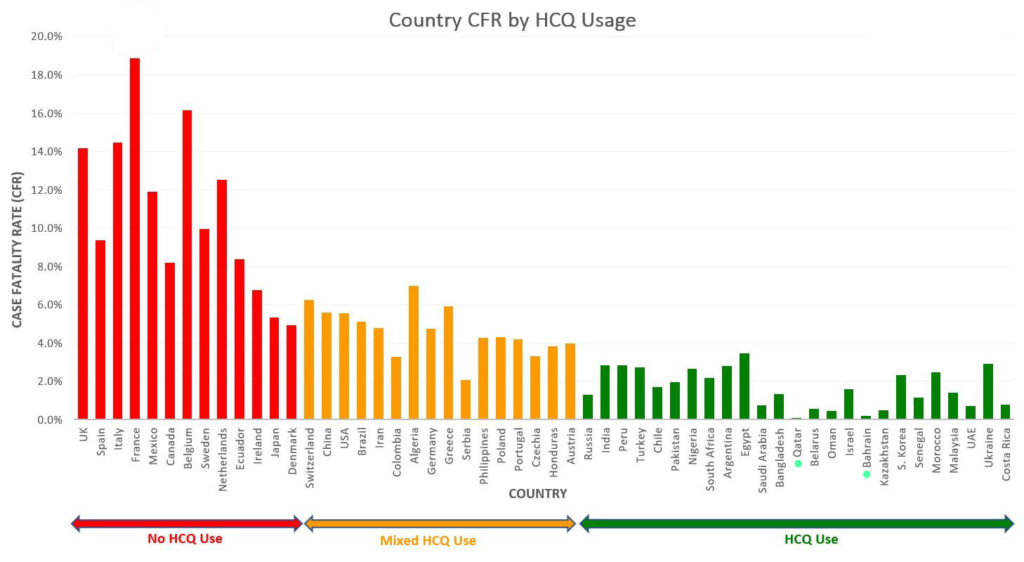
Why suppress an apparent miracle cure to fight COVID? Again, follow the money, not the science.
The NIH gave a non-recommendation for suspect reasons, while Pfizer and Merk stand to benefit by offering their own versions of the therapeutics. Presumably cash cows for the drug companies, Pfizer and Merck are sure to heavily market their new therapies across all media that are currently discounting IVM as little more than a horse dewormer, unsuitable for human consumption.
It can be assumed that there is no marketing budget to promote IVM. The Pfizer and Merck products, however, are sure to fit comfortably among the ad buys these companies place for the countless other remedies for all the other ailments we are besieged with daily across mainstream media.
Big Pharma is a cash cow for Big Media, and that cow will not be turned into burger.
Reuters, owned by the $40 billion international multimedia company, Thomson Reuters Corporation, is also in the business of “fact checking” social media posts. Reuters publishes its fact-checking commentary online in a format designed to resemble new stories, which turn up in online searches.
Jim Smith, who sits on Pfizer’s board, is also former president and current chairman of the Thomson Reuters Foundation, and CEO and director of Reuters parent company, Thomson Reuters Corporation. The conflict of interest is noteworthy.
Steve Kirsch, a Silicon Valley entrepreneur, has offered a $2 million prize to anyone who can provide a convincing argument that the NIH or WHO NEUTRAL and AGAINST recommendations on fluvoxamine or IVM (existing on May 21, 2021 when he made the offer) fit the evidence. To win the prize, Kirsch challenges contestants to convince him that:
- The NIH or WHO NEUTRAL and AGAINST rulings are more likely to fit the evidence than recommendations FOR these drugs, or
- The NIH or WHO NEUTRAL and AGAINST rulings are more likely to save more lives than recommending FOR these drugs.
Thus far, the prize has gone unclaimed.

But the battle against IVM is not just about pushing competing therapeutics—it goes well beyond that. Parents might be surprised to discover that an EUA is granted only in the event that there are no adequate, approved, and available alternatives for treatment. Thus, if IVM was recognized as such an alternative, it would cost the entire clown show billions in revenue.
The Company Behind the Curtain
Make no mistake, Big Pharma is not in the business of saving lives. That is a byproduct of the industry’s true objective—making money. Which is not to say that there aren’t brilliant and caring employees within the industry who truly care about humanity—and it is for the sake of humanity that these people are encouraged to become whistleblowers.
In an impassioned plea for whistleblowers to come forward and expose the dangers of the experimental serums, The Highwire has issued the $1 Billion Whistleblower Search.
Consider the alleged leaked, secret contract between Pfizer and the Government of Albania, one of many such deals inked with governments throughout the world. Posted by Twitter user Ehden, an information security and privacy professional based in the United Kingdom, Pfizer’s contract with Albania reveals the following:
- Even if a drug will be found to treat COVID19 the contract cannot be voided.
- The purchaser acknowledges the long-term effects and efficacy of the vaccine are not currently known and that there may be adverse effects of the vaccine that are not currently known.
- The purchaser hereby agrees to indemnify, defend and hold harmless Pfizer, BioNTech (and) their affiliates from and against any and all suits, claims, actions, demands, losses, damages, liabilities, settlements, penalties, fines, costs and expenses.
- Pfizer shall also have the right to assume control of such defence and the purchaser shall pay all losses, including, without limitation, the reasonable attorneys’ fees and other expenses incurred.
In an impassioned speech, Romanian MEP Cristian Terhes calls out the lack of transparency from the vaccine manufacturers, even displaying redacted pages from the contracts to support his charges.
To put things in financial perspective, inoculations were sold for $12 per shot to Albania, $19 per injection in the US, and $62 per dose in Israel (Oy!).
In Bangladesh, IVM costs $1.80 for an entire 5-day course.
Furthermore, a recent undercover video from Project Veritas reveals Brandon Schadt, Johnson & Johnson Regional Business Lead, weighing in on his company’s product as it relates to children.
“It’s a kid, you just don’t do that, you know? Not something that’s so unknown in terms of repercussions down the road, you know?” Schadt said.
“It’s a kid, it’s a f*cking kid, you know? They shouldn’t have to get a f*cking [COVID] vaccine, you know?”
Threat Assessment
But even if a parent’s child was to contract COVID, research from Kings College London has found that, on average, children between five and 11 years-old recovered in just five days, and the illness lasts for about seven days in kids between 12 and 17.
Lingering side-effects of the infection, also known as “Long COVID,” occurred in just 4.4% of patients after one month. A mere 1.8% experienced long COVID symptoms two months later.
It is not the experimental serum that will help children fight off the disease. COVID injections only tamp down symptoms of infection in much the same way cold and flu medicines may help subdue a cough or reduce fever.
There has been found to be no significant difference in viral load between vaccinated and unvaccinated, asymptomatic and symptomatic groups when infected with SARS-CoV-2 delta variant. But infected inoculated individuals are more likely to spread COVID. This is because with suppressed symptoms, these individuals will be more likely to treat the infection as if it were a cold, going out in public and taking fewer precautions to avoid contaminating others.
From as early as March 2020, studies done in Italy were suggesting 50-75% of positive Covid tests had no symptoms. Another UK study from August 2020 found as much as 86% of “Covid patients experienced no viral symptoms at all.
A large study in the UK found that people with a history of SARS-CoV-2 infection experienced greater rates of side effects following inoculation than those who had not previously contracted the disease.
Children, however, have a natural protection—they do not have the molecular and biological basis like adults, who are at greater risk to be infected and to become severely ill. This natural defense obviates the need for any perceived protection afforded by any unproven serum.
On the 3rd September 2021 the Joint Committee on Vaccination and Immunisation (JCVI) announced they were not recommending the Pfizer Covid-19 injection be offered to all children over the age of 12.
The JCVI determined that, “For the vast majority of children, SARS-CoV-2 infection is asymptomatic or mildly symptomatic and will resolve without treatment. Of the very few children aged 12 to 15 years who require hospitalisation, the majority have underlying health conditions.” Again, a child’s natural defenses are preferable to injection of an experimental agent.
Natural Immunity
There is a growing body of evidence to suggest that infection and the development of an antibody response (natural immunity) provides protection similar to or even better than currently used COVID inoculations, especially for children.
A recent report by the New York Times, showed that people who have been naturally infected with coronavirus have natural immunity that will likely last for years, and maybe forever.
“After infection, most people who have recovered still have enough immune cells to fend off the virus and prevent illness, the new data show. A slow rate of decline in the short term suggests, happily, that these cells may persist in the body for a very, very long time to come,” the New York Times reports.
A new study from Harvard tracked vaccinated and unvaccinated Massachusetts healthcare workers and showed 0 infections in 74,557 person-days for previously infected patients compared to 49 infections out of 830,084 person-days for fully vaccinated patients.
In short, if you’ve recovered from COVID, it is completely nonsensical for you to be vaccinated. You have virtually no chance of being re-infected.
- Recovered patients much more protected from re-infection than vaccinated patients
- Recovered patients, even if they get COVID, cannot pass it on to anyone else as far as we know (as the CDC was forced to reveal under FOIA from Aaron Siri)
- We don’t know if subsequently getting vaccinated after recovering will improve or degrade points 1 or 2
COVID serum-induced immunity focuses on the spike protein—only one portion of the virus. Once that portion of the virus has mutated sufficiently, the vaccine no longer is effective.
Natural immunity, however, focuses on the entire virus. Boasting a more diverse array of antibodies and T-cell receptors, your body’s built-in defenses will provide better protection overall, as it has more targets in which to attack the virus.
After the body has fought off an infection or disease, a small number of memory T cells, which are a type of white blood cell, are the first responders of the adaptive immune system. Their job is to remember how to ward off these invaders if they ever return. They kickstart antibody production, as well as target and destroy harmful viruses and bacteria. T cells persist in the blood long after antibody responses wane.
In his piece titled Science Catches Up — And Burns You All, author Karl Denninger distills data contained within a paper in the journal Nature. Denninger writes, “In 100% of the persons who had and recovered from Covid-19 and 81% of those who have never had the virus, a vaccine may well be worthless as they already have T-cell response.”
“The entire premise of all of the ‘mitigations’ and demand for mass-vaccination relied on a lie; that this was a ‘novel’ virus to which nobody had existing resistance,” Denninger continues.“We now know that’s false; 81% of the population in fact does have existing immunity and further, that immunity is strengthened, materially so, by natural infection . . . The existing vaccines are worthless for building said perfected immunity since the data is that the nucleocapsid section, which the vaccines do not code, is where most of the pre-existing resistance against serious disease resides . . . What we are doing now is encouraging more-contagious mutation and if we don’t cut it out we may well pull the black ball and get the more-virulent mutation as well that will evade all those who are vaccinated and hammer the hell out of them since none got any nucleocapsid T-cell recognition from the shot!”
In his The Chloroquine Wars essay, Matthew Crawford writes, “So far, popular vaccines do not seem to be resulting in much T cell immunity: just 31% among those who receive the AstraZeneca vaccine and 12% among those who receive the Pfizer vaccine. These vaccines seem to depend on B cell antibody emission to fight COVID-19. Antibodies aren’t nearly as long lived as T cells, the latter of which may be more responsible for immunity to SARS-CoV-2 in particular (also here).”
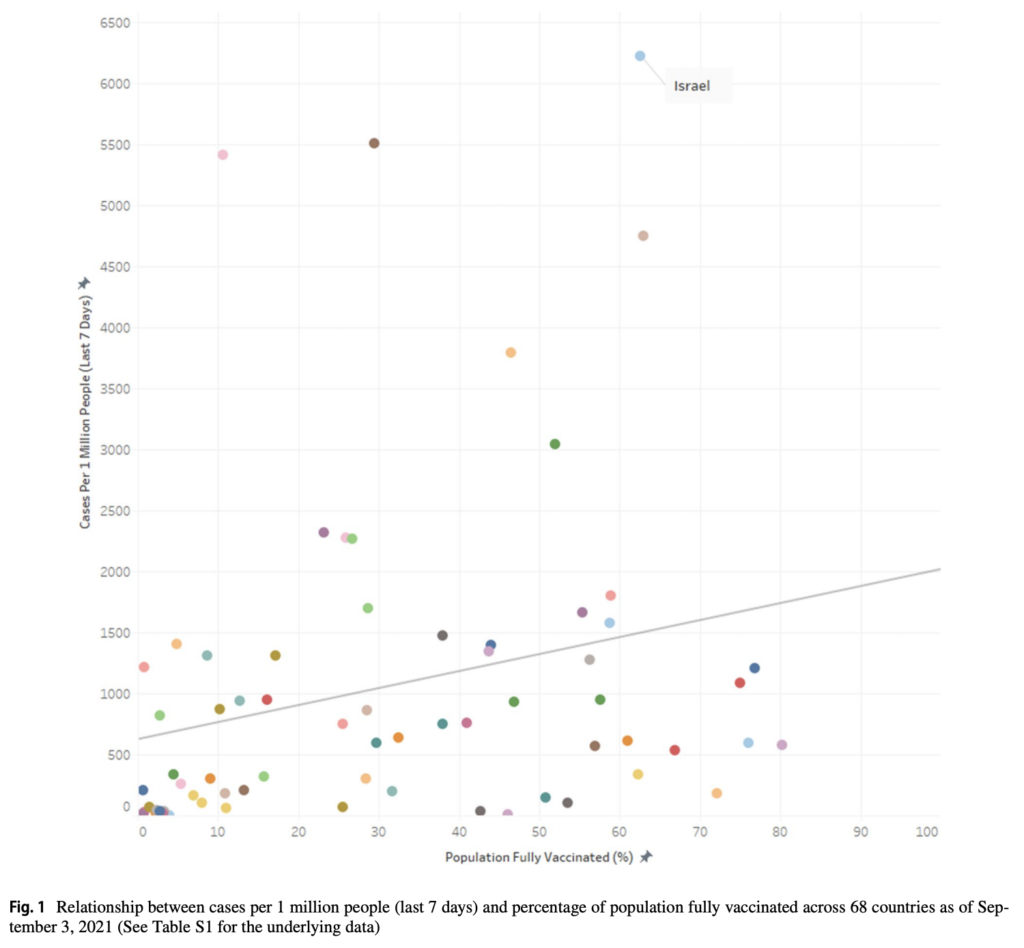
A recent study from A Harvard population health geographer and student researcher out of Canada examined 68 countries. They found that counties with higher percentage of population fully inoculated have higher COVID-19 cases per 1 million people. Using Israel as an example, the authors demonstrate how over 60% of that Mideastern population—fully inoculated—“had the highest COVID-19 cases per 1 million people in the last 7 days.”
Furthermore, Iceland and Portugal, with each nation having 75%+ of the population fully vaccinated, experienced greater numbers of COVID cases per 1 million than nations such as Vietnam and South African, which only had 10% of their respective populations immunized against COVID.
In a Project Veritas exposé, Pfizer scientists even admit natural immunity is more effective than their inoculations. Chris Croce, a Pfizer Senior Associate Scientist, can be heard to confess, “You’re protected for longer” if you have natural COVID antibodies compared to the COVID vaccine.
Even the CDC has been forced to admit to the lie of a pandemic of the unvaccinated. While you would assume that the CDC would have proof of at least one instance of an unvaccinated, naturally immune individual transmitting the COVID-19 virus to another individual, they have no such evidence.
When attorney Aaron Siri’s firm, on behalf of ICAN, submitted a FOIA to the CDC for precisely this proof, the CDC responded that it does not have a single document reflecting that this has ever occurred. Not one.
Siri notes, “In contrast, there are endless documents reflecting cases of vaccinated individuals becoming infected with and transmitting the virus to others. Such as this study. And this study. And this study. And this study. It goes on and on…”
“But it gets worse. The CDC’s excuse for not having a shred of evidence of the naturally immune transmitting the virus is that “this information is not collected.” What?! No proof! But yet the CDC is actively crushing the rights of millions of naturally immune individuals in this country if they do not get the vaccine on the assumption they can transmit the virus. But despite clear proof the vaccinated spread the virus, the CDC lifts restrictions on the vaccinated?! That is dystopian.”
Waning Effectiveness
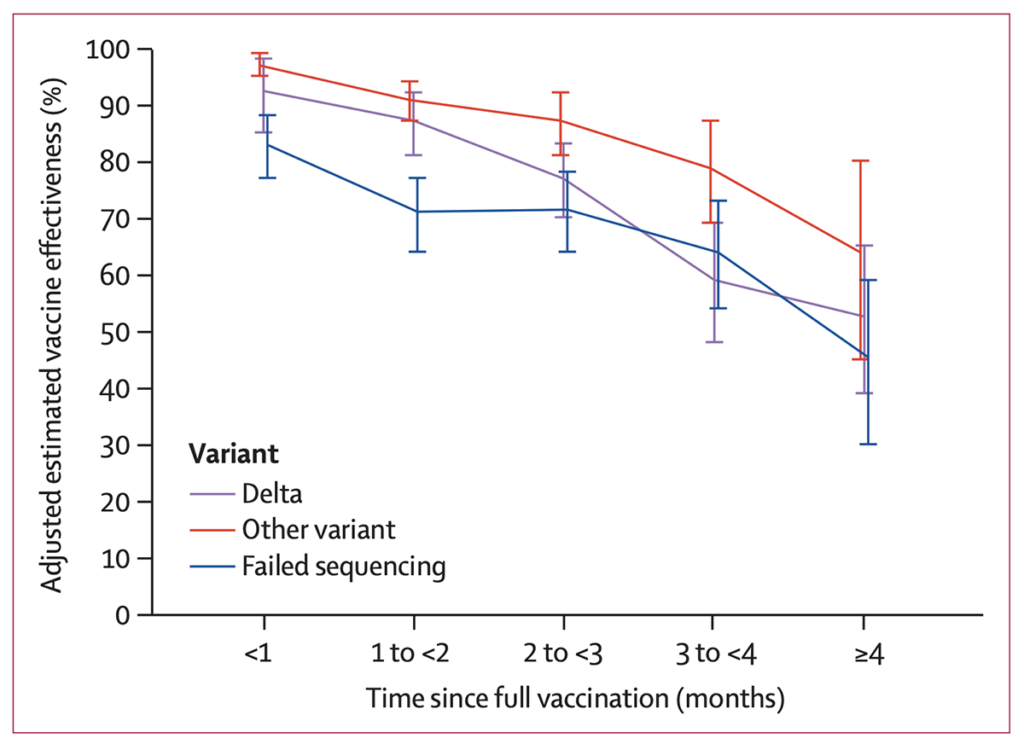
In terms of effectiveness, It’s been found that Experimental serum effectiveness wanes over a relatively short period of time. The effectiveness against delta infections at one month after being fully inoculated was high at 93% (85–97) but fell to 53% (39–65) up to 5 months after being fully inoculated. Effectiveness against other (non-delta) variants within one month of being fully inoculated was also high at 97% (95–99) and also waned, to 67% (45–80) up to five months after being fully inoculated.
As reported through CNN, another study found that among more than 600,000 veterans, J&J’s vaccine’s protection fell from 88% in March to 3% in August. Meanwhile, Moderna’s vaccine protection against infection fell to 64% from 92%, and Pfizer’s declined to 50% from 91% during that same time period.
Boosters are be needed to recharge any perceived or real protection afforded by these inoculations. What are the cumulative effects of these injections on a patient’s body? We have no data to answer this. But we do know that the definition of insanity is doing the same thing over and again while expecting a different outcome.
Natural Immunity vs Vaccine-Induced Immunity
Researchers from the University of California, Los Angeles, (USC) University of Southern California (USC), and the Cleveland Clinic conducted a meta-analysis of studies probing the risk associated with SARS-CoV-2 reinfection among those previously infected with SARS-CoV-2. The authors discovered that natural immunity appears to last at least ten (10) months. They also conclude, “The Protective effect of prior SARS-CoV-2 infection on re-infection is high and similar to the protective effect of vaccination.”
Traditional vaccines, such as those for influenza, use an inactivated virus that was destroyed by heat or chemicals to elicit an immune response without infecting the recipient. Others, such as for measles or mumps, use a weakened virus that is unable to hurt you but can still train your immune system to fight it.
When you get a traditional vaccine, your immune system responds to the foreign molecules that make up any vaccine via two different systems.
- The initial response uses your body’s innate immune system to summon white blood cells called neutrophils and macrophages to travel to the threat and work to destroy it. This system is activated as soon as your cells notice you’ve been exposed to any foreign material, from a bullet to a virus. This first line of defense is relatively ephemeral, and can last for several hours or days
- The second line of defense is an adaptive response, and takes days to weeks to set into motion. This long-lasting response relies on your immune system’s T and B cells that learn to recognize specific threats, such as a protein from the coronavirus. If the threat is encountered again, months or even years in the future, it’s these immune cells that will remember the old enemy and start generating the antibodies that will work to destroy it.
The Spike Protein
It has been discovered that the spike protein generated by the COVID serums is actually toxic. It is the cause of the vascular, neurodegenerative issues, not the virus. Some people produce more spike protein than others, however, which is why most people are not seriously affected.
While spike was meant to remain at the point of inoculation (the shoulder muscle), research shows that it travels to many organs of the body, including the brain, heart, ovaries, etc., causing severe damage. Researchers found that the spike it enters the blood stream within days of inoculation, and accumulates in spleen, brain, bone marrow, liver, adrenal glands, with high concentrations in ovaries. Furthermore, when in circulation, it binds to platelets, epithelial cells of blood vessels—causing clotting, bleeding, heart problems, brain blood clotting.
“We made a big mistake, and didn’t realize it till now,” said Professor Bryam Bridle, a vaccine researcher who was awarded a $230,000 government grant for research on COVID vaccine development. “We thought the spike protein was a great target antigen but never knew the spike protein itself was a pathogenic toxin protein.” “By vaccinating people we are inadvertently inoculating them with a toxin.”
To sum up, not only is the COVID serum largely ineffective at keeping recipients from acquiring and/or transmitting COVID, but evidence indicates that it degrades the immune system, while the generated spike protein causes death and injury.
Viral Evolution
Because the goal of a virus is to replicate and spread, if it kills its host, the objective cannot be fulfilled. That is why most viruses will affect the host with symptoms generally mild enough to survive infection with little difficulty. A virus such as Ebola, however, will kill the host—and in doing so become less transmissible. Thus, the virus will evolve to become less, not more virulent in order to afford itself better opportunity to replicate and transmit to other hosts.
But what if a host can carry a typically lethal virus without succumbing to the invader? What if the host is able to merely suppresses the deadly effects of the virus without actually killing the microbe? And what if the inoculated host is not only able to infect and replicate but also transmit the lethal disease to others? Then the disease will benefit from a huge boost in propagation while evolving into even more virulent strains as it adapts to escape the dampening effects of inoculation.
This is the unfortunate and deadly consequence of deploying a “leaky” solution. It is the classic Darwinian principle of natural selection played out virally.
A leaky vaccine is one that prevents severe infection and perhaps death, but it does not stop viral replication and transmission. With suppressed symptoms, the vaccinated become unaware super spreaders, leading to a possible/probable surge in overall fatality rates.
A “sterilizing” vaccine, on the other hand, is one that sets up lifelong immunity that never wanes and blocks both infection and transmission. Childhood vaccines for polio, measles, mumps, rubella and smallpox aren’t leaky; they are considered sterilizing treatments. As such, they are in no way in danger of falling prey to the phenomenon described with leaky products.
In his piece “Why are the current Covid-19 mass vaccinations to be considered a public health experiment,” Virologist Geert Vanden Bossche (DMV, PhD), writes, “Mass vaccination with imperfect vaccines is prone to promoting propagation of naturally selected, spike(S)-directed immune escape variants in the population, and ongoing campaigns are causing the population to place even more pressure on viral infectiousness.”
“This is, therefore, likely to expedite the already worrisome evolution of mutants into immune escape variants that further resist neutralizing vaccinal Abs while also presenting other problematic characteristics such as enhanced infectiousness or virulence. It goes without saying that such ‘super variants’, as molecular epidemiologists tend to call them, bear life-threatening potential to both unvaccinated and vaccinated individuals.”
The UK Health Security Agency published a report noting that vaccinated people don’t seem to be producing antibodies to the nucleocapsid protein, the shell of the virus, which are a crucial part of the response in unvaccinated people. Author Alex Berenson explains, “This means vaccinated people will be far more vulnerable to mutations in the spike protein EVEN AFTER THEY HAVE BEEN INFECTED AND RECOVERED ONCE (or more than once, probably).”
In recognizing the COVID inoculations’ failure to meet the medical standard of vaccine immunity, the CDC updated its definition on Sept. 1.
The definition of “vaccine” was formerly, “a product that stimulates a person’s immune system to produce immunity to a specific disease, protecting the person from that disease.” It is now, “A preparation that is used to stimulate the body’s immune response against diseases.”
Much simpler to redefine the product then it is to reformulate it to meet the standard.
But breakthrough cases have become increasingly difficult to ignore, and the failure of the COVID products are becoming increasingly apparent. So, expectations must be lowered among a populace that is beginning to take notice.
In addressing the apparent failure of the COVID inoculations to live up to its original promise of immunity, FingerLakes1.com reported, “What’s most important to know is that everyone will likely become infected with the virus at some point, but it’s important to be vaccinated so the infection is mild and lowers the possibility of hospitalization or death.”
Think about that. By any measure, is what they’re describing really a vaccine at this point, or is it therapy? You can accomplish the same results via vitamin D, zinc, HCQ, IVM, etc. All of these therapeutics have proven to lower the possibility of hospitalization or death, but without the associated risk of potential side effects, death, or cost—both financial and emotional.
According to virologist and inventor of mRNA technology Robert Malone, “The difference in the efficacy regarding how traditional live-attenuated vaccines work, (such as Polio, Yellow Fever, and Smallpox,) as opposed to mRNA vaccines, is that the former are administered prior to a major outbreak, preventing opportunity to spread. But once the virus is already embedded into a large fraction of the population, that logic fails. Ultimately, vaccinating during an outbreak drives more potent mutations.”
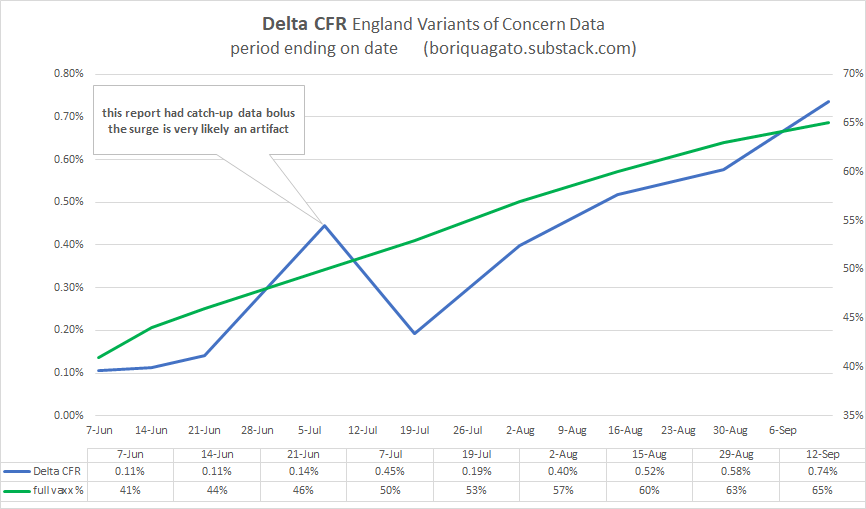
In his substack entry titled, are leaky vaccines driving delta variant evolution and making it more deadly? assessing the england data on variants and vaccines. the pieces are coming together, el gato malo writes, “none of the other variants (pre vaccine) worked like this. none saw CFR [case fatality rate] rise like this. and no jump from major variant to variant saw a statistically significant rise in deadliness. this IS however what one would expect if a virus were undergoing vaccine mediated evolution (as mareks disease did in chickens) and selecting for hotter strains because vaccinated people can carry and spread them and not die.”
Among other pieces of evidence, malo presents the following chart to buttress his theory of vaccine mediated evolution (VME) in England.
The theory of VME can be detected in other countries, as well. Israel in particular is being closely watched now because it was one of the first countries to begin a mass vaccination campaign, beginning in December 2020. The country has among the world’s highest levels of vaccination for COVID-19, with 60-80% of those 12 and older fully vaccinated, the vast majority with the Pfizer vaccine. Yet, the Israel is now recording one of the world’s highest infection rates.
Consider the chart below, with observations provided by Dr Peter A.McCullough. They appear in his article titled “Israel’s Booster Program’s Not Stopping Sky Rocketing Cases and Higher Number of Deaths—What’s Going On?”
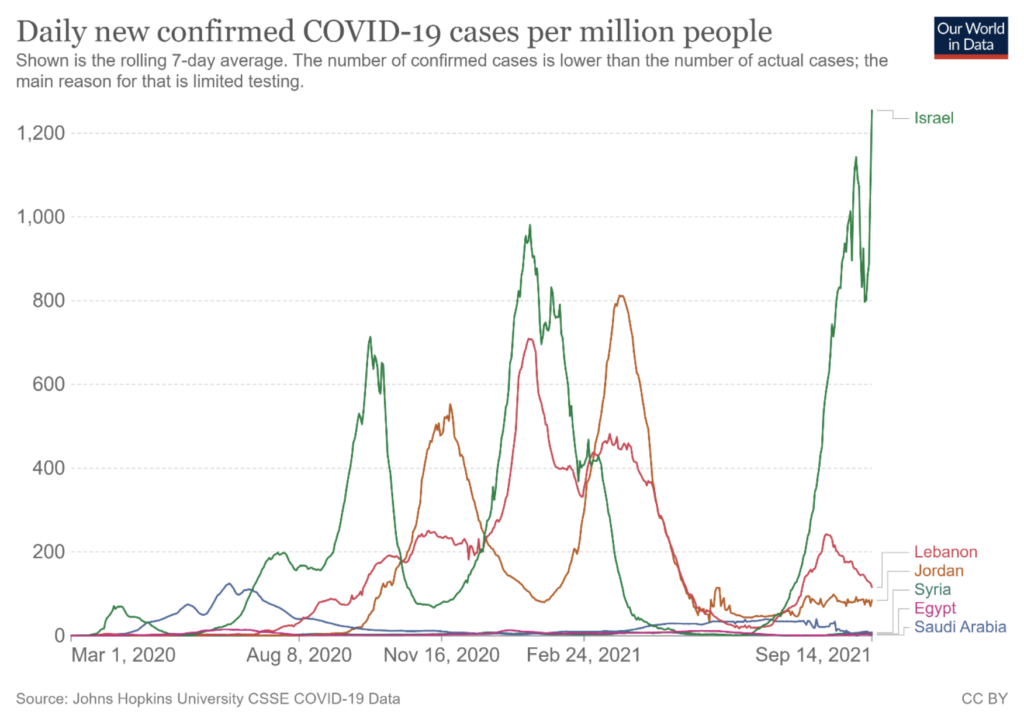
The graph has three key points:
- The surge in infections in Israel post 3rd booster start Aug 1st 2021 is greater than the peak seen in the prior highest level (green dotted line, January 18th, 2021).
- You can see that from August 1st 2021 to Sept 14th 2021, the infections are sky rocketing and the key issue is that the booster program was started on August 1st. It has failed. It is likely that the vaccinated are carrying the Delta and participating in the transmission of it and fueling the transmission and it can be argued that the booster is driving this.
- If you look at Israel and compare it to other middle eastern nations, you see the clear difference in infections and especially how Aug 1st 2021, their infections are going down while Israel’s escalated up and mainly due to the booster initiation.
Following up on COVID cases in Israel, a montage of COVID deaths graphed by country pre and post-inoculation can be seen below.
85% of the population of Singapore are fully inoculated with COVID serum. Furthermore, the country has instituted a version of zero-tolerance COVID-19 policy in place for over a year—that is, tight border controls, frequent testing, proactive contact tracing. According to Reuters, nearly 70% of all deaths reported in the nation have been recorded since August—a time when well over 75% of the country’s population was inoculated.
Given the evidence, a strong argument can be made that we are not experiencing a “Pandemic of the unvaccinated,” but rather a “Pandemic of the vaccinated.”
Risk-Benefit Assessment
Taking everything above into account, we’ll put some data into a risk-benefit table:
| If a Child DOES GET Inoculated | If a Child DOES NOT GET Inoculated | |
|---|---|---|
| Risk of Contracting COVID | Yes | .9%1 |
| Risk of transmitting COVID | Yes2 | Yes2 |
| Risk of hospitalization from COVID | Yes | .056%3 |
| Risk of long COVID (>8 weeks) | 1.8% | 1.8%4 |
| Risk of death associated with COVID | Yes | .000235714%5 |
| Risk of degrading innate immune system | Yes6 | None |
| Need for frequent booster shots (while compounding associated risks) | Yes | None |
| Risk of hospitalization due to inoculation (12-17 year-old male) | 3-5 times more likely than Covid hospitalization7 | None |
| Risk of death due to inoculation (12-17 year-old male) | 16% more likely than from Covid death7 | None |
| Risk of damage from inoculation appearing in intermediate to long term future | Yes8 | None |
| Risk of user (not drug manufacturer or agents) being responsible for any and all damages resulting from inoculation | 100% | None |
- Susceptibility to SARS-CoV-2 Infection Among Children and Adolescents Compared With Adults (I adjusted the study’s .56 figure upward by 60% to account for greater transmissibility of delta variant)
- No Significant Difference in Viral Load Between Vaccinated and Unvaccinated, Asymptomatic and Symptomatic Groups When Infected with SARS-CoV-2 Delta Variant
- For 5-17 year-olds, according to CDC data
- Long COVID uncommon in children, analysis finds
- According to CDC’s own slide, presented at ACIP Meeting November 2, 2021 at the CDC
- Test of diabetic’s blood pre and post-inoculation revealed dramatic decline in patient’s immune system (video)
- For 12-15 year-olds, based on actuary calculations
- According to the trial schedule for the FDA-approved Pfizer serum, the latest we should expect to have a final study report (potential long term effects) submitted to the FDA would be May 31, 2027. The earliest final report (efficacy study) is not due for submission until June 30, 2023!
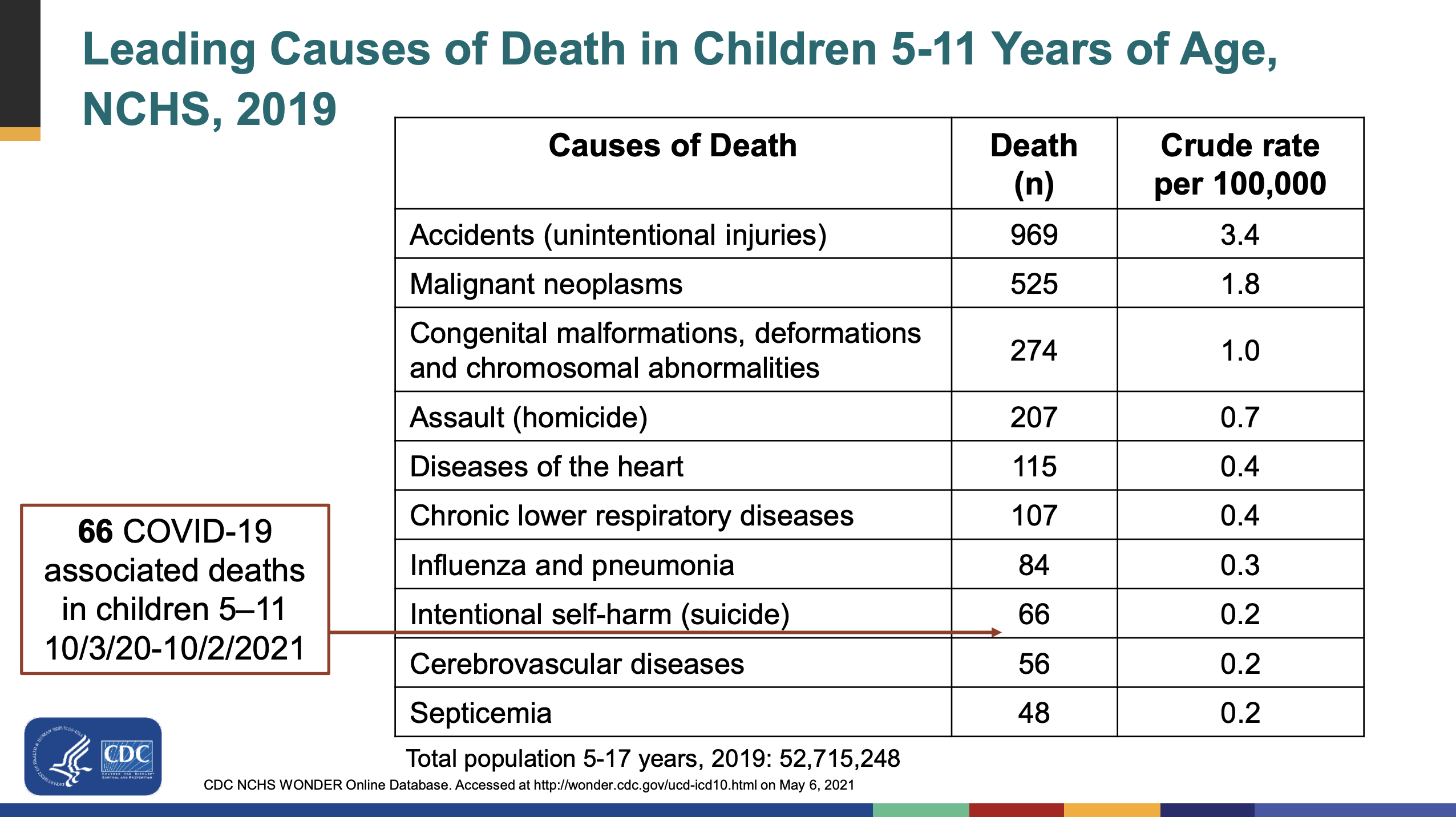{kind=link}
{kind=link}
Wonderful, what a webpage it is! This weblog provides useful
facts to us, keep it up.